Penicillin Hypersensitivity
Download / Print Section as PDFPenicillin Hypersensitivity
-
The risk of penicillin hypersensitivity is an important one, as anaphylaxis can be fatal. On the other hand, avoidance of penicillin because of concerns regarding allergy is widespread, and in many situations unnecessary. This leads to increased use of broad spectrum antimicrobials which contributes to development of antimicrobial resistance, and is associated with higher morbidity and mortality in these patients (e.g. suboptimal therapy, C. difficile infection), longer hospital stay and higher healthcare costs. The HSE have useful information on prescribing in patients with penicillin allergy .
-
An accurate patient history is important when evaluating allergy. Important details of an allergic reaction include signs, symptoms, severity, timing of onset of the reaction in relation to drug exposure, antimicrobial agent and administration route used, date of event, prior reactions, subsequent exposure to same or related agents, other medicines being taken concurrently, time and route of their administration, and adverse drug reactions to other medicines.
-
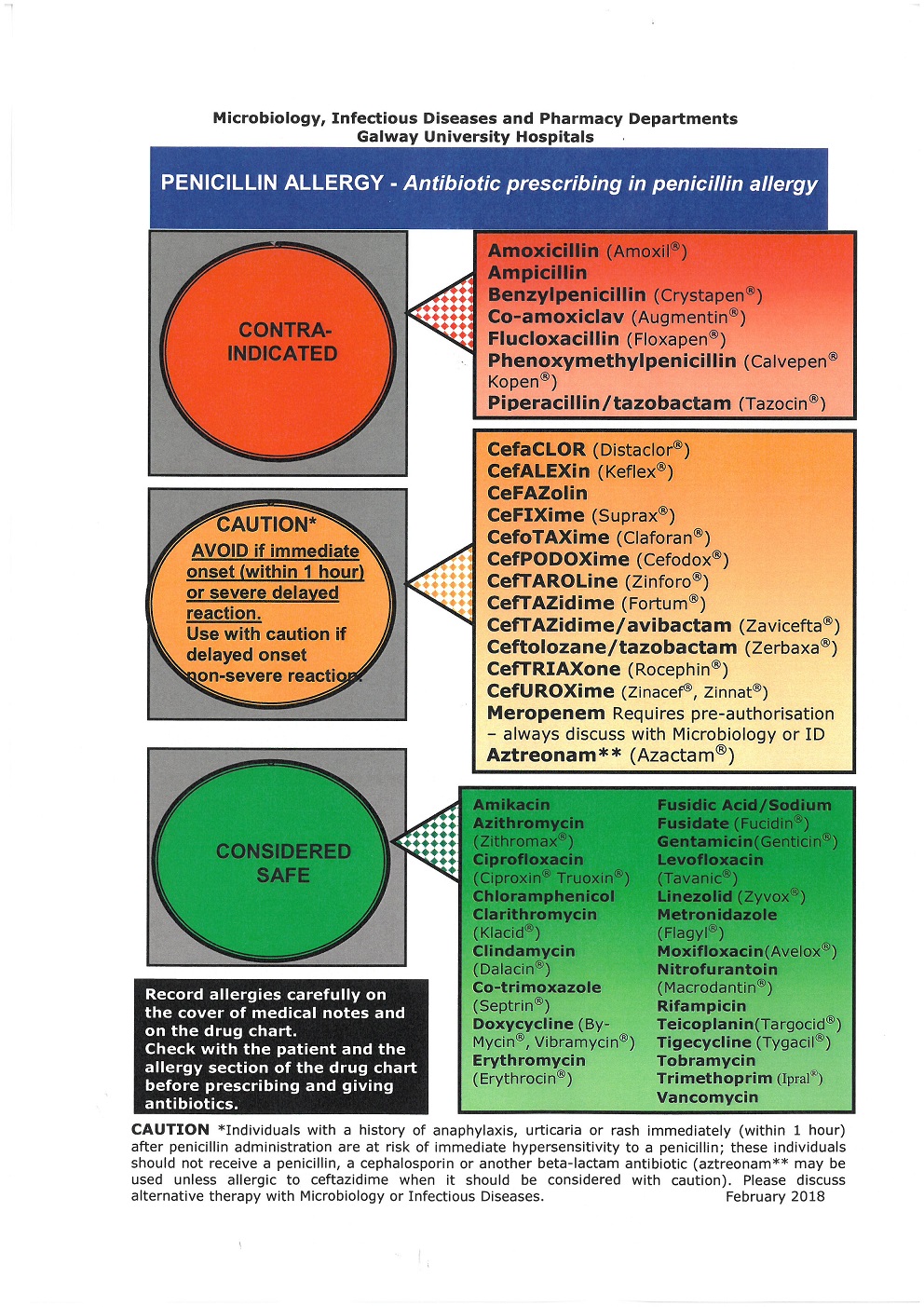
Record allergies carefully in the medical notes and on the drug chart including date and nature of reaction and your signature and MCRN.
-
Transfer allergy information when re-writing the drug chart.
-
Check with the patient and the allergy section of the drug chart prior to prescribing and administering all antibiotics.
-
-
Assess reported symptoms critically to exclude non-allergic adverse reaction (e.g. diarrhoea, vomiting, non-specific maculopapular rash) or a reaction wrongly attributed to the antibiotic (e.g. treatment with amoxicillin is associated with rash in 80% of patients during Epstein-Barr virus infection). Do not document these as "allergies". If in doubt, consider consulting GUH Immunology.
3. For the purposes of prescribing in penicillin allergy it is important to differentiate between an
immediate hypersensitivity reaction, a severe delayed hypersensitivity reaction
and a
non-severe
delayed hypersensitivity reaction.
These are defined as:
-
Immediate - occurring within one hour of drug administration
-
Patients with a history of immediate (within one hour) hypersensitivity reaction (anaphylaxis, laryngeal oedema, bronchospasm, hypotension, local swelling, urticarial or pruritic rash) should not receive a penicillin, cephalosporin or carbapenem (e.g. meropenem) . If there is a compelling reason to consider the use of a beta-lactam agent in such a patient consult Microbiology, and contact the GUH Department of immunology who may be able to assist in assessing if the patient is likely to be hypersensitive to all beta-lactams.
-
-
Delayed - occurring more than one hour after drug administration
-
A minority of patients with a delayed hypersensitivity reaction will have a history of severe delayed hypersensitivity reaction (e.g. Stevens Johnson Syndrome (SJS), Toxic Epidermal Necrolysis (TEN), Drug Reaction Eosinophilic Systemic Syndrome (DRESS), Acute Generalised Exantematous Pustulosis (AGEP)). Patients with a history of severe delayed hypersensitivity reaction (SJS, TEN, DRESS, AGEP) to penicillin should not receive a beta-lactam – consultation with GUH Immunology/Dermatology advised.
-
Patients with a history of a non-severe rash with a delayed onset of more than one hour after penicillin administration may reasonably be prescribed a cephalosporin or carbapenem.
-
-
Patients for whom little or no information is available (after making every effort to determine allergy history), should not receive penicillin in the first instance but may be prescribed a cephalosporin or carbapenem with caution. Consider referral to GUH Immunology for further investigations.
-
The Penicillin Allergy Traffic Poster lists antibiotics that are contraindicated, can be used with caution and those that are considered safe to use in penicillin allergy.
-
Refer people with a suspected allergy to beta-lactam antibiotics to Immunology in GUH if they:
-
Need treatment for a condition that can only be treated by a beta-lactam or
-
Are likely to need beta-lactam antibiotics frequently in the future (e.g. those with anatomical predisposition to infections or immunodeficiency).
-
References:
- Demoly et al. International Consensus on drug allergy. Allergy 2014 (69) 420-437
- Shenoy et al. Evaluation and management of penicillin allergy. JAMA 2019;321(2):188-199
- www.antibioticprescribing.ie
- Drug allergy: diagnosis and managements. NICE clinical guidelines 2014. https://www.nice.org.uk/guidance/cg183 (Revised in 2018)