Pdf is being generated, will be available at /media/pdfs/meg-demo-meg-staff-app-helicobacter-pylori.pdf shortly
Helicobacter pylori
Download / Print Section as PDF
The second Irish Helicobacter pylori Working Group consensus for the diagnosis and treatment of Helicobacter pylori infection in adult patients in Ireland
Sinéad M. Smitha, *, Breida Boyleb, Martin Buckleyc, Conor Costigana,d, Maeve Doylee, Richard Farrellf , M. Syafiq Ismailg, David Kevansa,h, Sean Nugenti , Anthony O’Connora,d, Colm O’Moraina, Vikrant Pariharj , Cristín Ryank and Deirdre McNamaraa,d, *
Background
There has been an increase in resistance to many of the antimicrobials used to treat Helicobacter pylori (H.pylori) nationally and internationally. Primary clarithromycin resistance and dual clarithromycin and metronidazole resistance are high in Ireland. These trends call for an evaluation of best-practice management strategies.
Objective
The objective of this study was to revise the recommendations for the management of H. pylori infection in adult patients in the Irish healthcare setting.
Methods
The Irish H. pylori working group (IHPWG) was established in 2016 and reconvened in 2023 to evaluate the most up-to-date literature on H. pylori diagnosis, eradication rates and antimicrobial resistance. The ‘GRADE’ approach was then used to rate the quality of available evidence and grade the resulting recommendations.
Results
The Irish H. pylori working group agreed on 14 consensus statements. Key recommendations include (1) routine antimicrobial susceptibility testing to guide therapy is no longer recommended other than for clarithromycin susceptibility testing for first-line treatment (statements 6 and 9), (2) clarithromycin triple therapy should only be prescribed as first-line therapy in cases where clarithromycin susceptibility has been confirmed (statement 9), (3) bismuth quadruple therapy (proton pump inhibitor, bismuth, metronidazole, tetracycline) is the recommended first-line therapy if clarithromycin resistance is unknown or confirmed (statement 10), (4) bismuth quadruple therapy with a proton pump inhibitor, levofloxacin and amoxicillin is the recommended second-line treatment (statement 11) and (5) rifabutin amoxicillin triple therapy is the recommend rescue therapy (statement 12).
Conclusion
These recommendations are intended to provide the most relevant current best-practice guidelines for the management of H. pylori infection in adults in Ireland. Eur J Gastroenterol Hepatol XXX: XXXX–XXXX
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
European Journal of Gastroenterology & Hepatology XXX,
XXX:XXXX–XXXX
Keywords: antimicrobial resistance, bismuth, clarithromycin, consensus guidelines, Helicobacter pylori, levofloxacin, quadruple therapy, rifabutin, tetracycline, triple therapy
a
School of Medicine, Trinity College Dublin,
b
Department of Clinical Microbiology, St. James’s Hospital, Dublin,
c
Department of Gastroenterology, Mercy University Hospital, Cork,
d
Department of Gastroenterology, Tallaght University Hospital, Dublin,
e
Department of Microbiology, University Hospital Waterford, Waterford,
f
Department of Gastroenterology, Connolly Hospital, RCSI, Dublin,
g
Department of Gastroenterology, Cavan and Monaghan Hospital,
h
Department of Gastroenterology, St. James’s Hospital, Dublin,
i
Department of Gastroenterology, Whitfield Clinic, Waterford,
j
Department of Gastroenterology, Letterkenny University Hospital, and
k
School of Pharmacy and Pharmaceutical Sciences, Trinity College Dublin, Dublin, Ireland
Correspondence to Sinéad M. Smith, PhD, Trinity Academic Gastroenterology
Group Research Centre, Rm 1.46 Department of Clinical Medicine, Trinity
Centre, Tallaght University Hospital, Dublin 24, Ireland
Tel: +353 1 896 3844; fax: +353 1 896 2988; e-mail: smithsi@tcd.ie
This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal.
*Sinead M. Smith and Deirdre McNamara contributed equally to the writing of
this article.
Received
25 January 2024
Accepted
8 May 2024.
0954-691X Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Introduction
The Gram-negative bacterium Helicobacter pylori (H.pylori) infects the stomach of almost 50% of individuals globally and causes chronic gastritis. In 2015, the KyotoH. pylori consensus defined H. pylori gastritis as an infectious disease [1]. Although chronic active infection leads to structural and functional changes in the gastric mucosa, most individuals remain asymptomatic [2,3]. H. pylori
infection increases the risk of developing peptic ulcers, gastric adenocarcinoma and gastric mucosa-associated lymphoid tissue lymphoma and has been grouped as a class I carcinogen by the WHO [4]. Vitamin
B12
deficiency, unexplained iron-deficiency anaemia and certain cases of idiopathic thrombocytopenic purpura are also associated with H. pylori infection [2,3]. While the prevalence of H.pylori has decreased in many parts of the world [5], the management of H. pylori infection remains a challenge. The Irish H. pylori working group (IHPWG) was established in 2016 and comprises gastroenterologists, micro-biologists and pharmacists with expertise in H. pylori
infection. The first consensus recommendations on the management of H. pylori infection specific to the Irish healthcare setting were published in 2017 [6]. Since then, many important updates have been published on the prevalence of H. pylori antimicrobial resistance and the eradication success rates of different treatment regimens. In light of these findings, international consensus guidelines
have been updated [3,7–10] Thus, the aim of this study was to reconvene the IHPWG to review the most up-todate literature relating to the management of H. pylori infection, together with national data on resistance rates and treatment outcomes, and provide revised recommendations most appropriate for the management of H. pylori in adult patients in Ireland.
Methods
Data review, assessment of evidence and revision of consensus statements
The IHPWG met on 22 June 2023, to discuss the recent literature and national data relating to the management of H. pylori. It was agreed that there was a need to update the Irish guidelines. Using a similar approach to that of the Maastricht VI guidelines [3], the Delphi process was used to develop revised consensus statements in relation to three key domains: diagnosis of H. pylori infection in symptomatic adults (domain 1), first-line treatment of H. pylori infection (domain 2) and second-line and rescue therapy for H. pylori infection (domain 3). First, this involved an in-depth review of the recent relevant national data, the published literature and current European and
international guidelines to identify the best evidence to support each recommendation. Revised recommendations were drafted and shared with the group. On 29 November 2023, group members were asked to vote on whether they agreed with each recommendation. If there was <80% agreement with the relevance of a recommendation, it was re-phrased, and another vote took place. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) [11,12] approach was used to rate the quality of the available evidence and the strength of the resulting recommendations according to the criteria in Table 1. Aspects related to the implementation of the recommendations in clinical practise in Ireland were also considered. The resulting recommendations are summarised in Table 2.
Recommendations
Domain 1: diagnosis of Helicobacter pylori infection in symptomatic adults
Statement 1: all patients with symptoms related to the upper gastrointestinal tract should be tested for Helicobacter pylori
Recommendation: strong; Quality of evidence: high. H. pylori eradication cures peptic ulcers in most patients whose ulcers are not associated with nonsteroidal anti-inflammatory drug use and reduces gastric cancer risk [13–22]. Eradication also leads to the regression of most localised gastric mucosa-associated lymphoid tissue lymphomas [23–26]. In addition, European guidelines recommend H. pylori eradication for patients with unexplained iron-deficient anaemia, idiopathic thrombocyto penic purpura and vitamin B12 deficiency [3]. For a number of years, European guidelines have recommended the test-and-treat strategy for the management of H. pylori by performing noninvasive testing of individuals with uninvestigated dyspepsia, followed by treatment in cases where H. pylori is detected [3,27,28]. The test-and-treat strategy is recommended in younger dyspeptic patients (<50 years) without alarm symptoms, such as weight loss, dysphagia, overt gastrointes tinal bleeding, abdominal mass or iron-deficient anaemia [3,27,28]. Options for noninvasive H. pylori testing include the urea breath test (UBT), the stool antigen test and serology. Endoscopy is recommended for those with dyspepsia symptom onset >50 years, those of any age with alarm symptoms or a family history of gastric cancer and all patients where the test-and-treat strategy fails [3,27,28]. H. pylori can be detected in biopsy samples taken during endoscopy using the rapid urease test (RUT), histology, culture and molecular methods such as the PCR.
Table 1. Criteria for assessing data quality and the strength of recommendations
|
Criteria for assessing data quality and the strength of
recommendations
|
|
Quality of evidence
|
|
Hight - Further research is very unlikely to change confidence in the estimate of the effect. Moderate - Further research is likely to have an important impact on confidence in the estimate of effect and may change the estimate. Low - Further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate. |
|
Strength of recommendation
|
|
Strong - Strong recommendation for using an intervention. Strong recommendation against using an intervention.
Weak - Weak recommendation for using an intervention. Weak recommendation against using an intervention. |
Statement 2: the urea breath test is the recommended noninvasive test for Helicobacter pylori. If the urea breath test is unavailable, the monoclonal stool antigen test is an alternative noninvasive test if locally validated
Recommendation: strong; quality of evidence: high. For the UBT, the patient ingests a solution containing
13
C-labelled (or less commonly
14
C-labelled) urea. The urease enzyme produced by H. pylori in infected patients converts the labelled urea to ammonia and labelled carbon dioxide, which is detected in a breath sample [29,30]. Bacterial antigens are present in the stool of individuals with active H. pylori infection [3]. The stool antigen test is an immunoassay that detects these antigens in stool samples [29]. Serological testing can detect IgG antibodies to H. pylori in the blood [29]. As the UBT is considered the most accurate noninvasive test for H. pylori [3] with high sensitivity and specificity values [31], it is the recommended noninvasive test in the Irish Healthcare setting. Current European guidelines recommend citric acid as the test meal because it slows gastric emptying and increases the distribution of the substrate and the contact time with H. pylori urease [3]. It is recommended that patients should fast in advance of the UBT.
|
Table 2.
Summary of consensus recommendations
|
|
Statements Strength Quality
|
|
Diagnosis of H. pylori infection in symptomatic adults
|
|
Statement 1
Strong High
All patients with symptoms related to the upper gastrointestinal tract should be tested for H. pylori.
Statement 2
Strong High
The UBT is the recommended noninvasive test for H. pylori. If the UBT is unavailable, the monoclonal stool antigen test is an alternative noninvasive test if locally validated.
Statement 3
Strong High
A combination of histology, taken from the antrum and corpus, and a RUT are recommended for invasive H. pylori testing.
Statement 4
Strong Moderate
A corpus and antrum biopsy sample should be taken for the RUT.
Statement 5
Strong Moderate
If H. pylori cultures are required, a corpus and an antrum biopsy should be taken.
Statement 6
Strong Moderate
AST by culture or a locally validated molecular method should be performed for national resistance surveillance and prior to prescribing clarithromycin-containing first-line therapy.
Statement 7
Strong High
Posteradication treatment testing must be performed. If gastroscopy is not required, a UBT is recommended for posteradication treatment testing. If the UBT is unavailable, the monoclonal stool antigen test is an alternative if locally validated.
Statement 8
Strong High
PPIs significantly reduce the accuracy of the recommended H. pylori tests; therefore, PPIs should be stopped 14 days before testing unless PCR testing is available.
|
|
First-line H. pylori therapy
|
|
Statement 9
Strong Moderate
14-day clarithromycin-based triple therapy with a high-dose PPI can only be recommended in cases where clarithromycin susceptibility has been confirmed.
Statement 10
Strong Moderate
Bismuth quadruple therapy with a high-dose PPI, metronidazole and tetracycline for 14 days is the recommended first-line treatment in the absence of clarithromycin susceptibility testing or where clarithromycin resistance has been confirmed. Although inferior eradication rates have been reported, doxycycline may be used if tetracycline is unavailable.
|
|
Second-line and rescue therapy
|
|
Statement 11
Strong Low
Bismuth quadruple therapy with a high-dose PPI, levofloxacin and amoxicillin for 14 days is the recommended second-line treatment. For those who received AST-guided clarithromycin first-line therapy a combination of PPI, bismuth, metronidazole and tetracycline can be given.
Statement 12
Strong Low
14-day rifabutin, amoxicillin triple therapy with high-dose PPI is the recommended rescue therapy. Alternatively, a combination of high-dose PPI and bismuth with 2 antibiotics not previously prescribed can be used.
Statement 13
Strong Low
For those with persistent H. pylori infection following unsuccessful eradication attempts, there is no current evidence-based guideline on appropriate follow-up. The IHPWG consensus is that endoscopic surveillance with ESGE-recommended mapping biopsies for precancerous changes should be considered at an interval of 5–10 years from last failed treatment.
Statement 14
Strong Moderate
As part of a quality assurance programme, H. pylori first-line, second-line and rescue therapy eradication rates should be locally monitored and audited as part of national and European registries.
|
AST, antimicrobial susceptibility testing; ESGE, European Society of Gastrointestinal Endoscopy; MAPS, Management of epithelial precancerous conditions and lesions in the stomach; PPI, proton pump inhibitor; Quality, quality of evidence; RUT, rapid urease test; Strength, strength of recommendation; UBT, urea breath test.
For stool antigen testing, potential options include laboratory-based enzyme immunoassays and more recently rapid immunochromatography-based tests for point-of-care diagnosis. In relation to laboratory-based tests, mAb-based assays are superior to polyclonal-based tests [32]. While studies evaluating rapid near-patient immunochromatography-based stool antigen tests are emerging, inferior performance compared to laboratorybased tests has been reported for primary H. pylori diagnosis [33–36]. Therefore, the monoclonal stool antigen test is recommended over both polyclonal laboratory-based tests and rapid immunochromatography-based assays. The monoclonal stool antigen test is considered an acceptable alternative to the UBT [3] and is an option in centres where the UBT is unavailable if the assay has been locally validated and is accredited by the Irish National Accreditation Board. Sample storage and transport procedures should be carefully considered when validating the monoclonal stool antigen test. Serology is more commonly used for H. pylori screening. There are a number of serology kits available commercially with varying performances [37]. Thus, any serological assay should be locally validated before
use. When serology is used as a test-and-treat strategy, a positive test should be confirmed by either the UBT or monoclonal stool antigen test before initiating H. pylori eradication therapy [3].
Statement 3: a combination of histology, taken from the antrum and corpus, and an rapid urease test are recommended for invasive Helicobacter pylori testing
Recommendation: strong; quality of evidence: high. While histological examination of biopsy samples requires highly trained personnel, it allows for the accurate detection of bacteria, staging of gastritis and examination of focal lesions [3,6]. To account for the patchy distribution of H. pylori, histological sampling should include two antrum biopsies (2–3 cm in front of the pylorus) and two corpus biopsies, which should be submitted in separate containers. Antral biopsies should be taken even if the mucosa looks healthy. An additional biopsy from the incisura is taken for gastritis histological staging when the OLGA (operative link on gastric atrophy) and OLGIM (operative link on gastric intestinal metaplasia) protocols are followed. Any focal lesions should be sampled [3]. Histochemical staining of the biopsy samples with hematoxylin and eosin or Giemsa identifies most cases of H. pylori. Immunohistochemical staining is recommended in cases of chronic active gastritis where H. pylori has not been detected by histochemistry alone. In cases of normal histology, immunohistochemical staining is not required [6,28]. The RUT is easy to perform, enables a quick diagnosis and allows for the immediate prescription of H. pylori eradication therapy [38]. Stomach biopsies are placed into a urea-containing medium within the well of a slide. If H. pylori is present within the tissue sample, the bacterial urease will break down the urea to generate ammonia, resulting in an alkaline pH, that is, detected by a pH reagent also present in the well [38]. Results from Tallaght University Hospital indicate that the sensitivity and specificity of the rapid urease test (TRI-MED Distributors, PTY LTD, Washington, USA) compared with histology are 80% and 90%, respectively [39]. Data from Connolly Hospital Blanchardstown indicate sensitivity and specificity values of 88% and 97%, respectively, for the Kimberly-Clark CLOtest (Ballard Medical Products, Utah, USA) and 78% and 97%, respectively, for the Quick Test (Biohit, Cheshire, UK) [40]. Therefore, the exclusive use of rapid urease testing forinvasive H. pylori diagnosis cannot be recommended [40].
Statement 4: a corpus and antrum biopsy sample should be taken for the rapid urease test
Recommendation: strong; quality of evidence: moderate. A biopsy from the antrum and the corpus should be taken for the RUT to account for the patchy distribution of H. pylori, which can occur due to proton pump inhibitor (PPI) use [38]. Emerging evidence from abroad and from Ireland suggests that testing the antrum and corpus biopsies either separately [41–43] or combined within the same test [44,45] significantly increases the diagnostic accuracy of the RUT. Additionally, the combined approach reduces the reaction time of the test, resulting in a more rapid diagnosis [44]. Accumulating evidence also supports the reuse of RUT biopsy samples for DNA isolation and the diagnosis of H. pylori infection by molecular methods such as PCR [46–49]. This eliminates the need to take additional biopsies specifically for PCR and provides the opportunity to perform antimicrobial susceptibility testing (AST) by analysing the H. pylori DNA for resistance-associated mutations (see statement 6). Another advantage of molecular methods for the detection of H. pylori is that they are less affected by PPI use than the other H. pylori detection methods [49–51]. Studies evaluating the feasibility and accuracy of reusing rapid urease test biopsies for PCR-based H. pylori detection and antimicrobial sensitivity testing are warranted in the Irish Healthcare setting.
Statement 5: if Helicobacter pylori cultures are required, a corpus and an antrum biopsy should be taken
Recommendation: strong; quality of evidence: moderate.The culture of H. pylori from biopsy specimens enables diagnosis and provides the opportunity for AST. While culture is very specific, it is time-consuming and requires expertise in the clinical microbiology laboratory [52]. Culture success rates range from as low as 55% to up to 93% [53,54]. Culture success is influenced by PPI use, the biopsy collection medium, sample transport conditions and contamination of the samples with other microorganisms. Dedicated biopsies should be taken from both the antrum and the corpus to increase culture success [55]. This recommendation has been supported locally by a study carried out at Tallaght University Hospital showing that H. pylori was successfully cultured in a significantly higher number of cases when combined antrum and corpus biopsy sampling was used compared with a single antrum biopsy [64.4% (n = 94/146) vs. 49.3% (36/73); P = 0.04)] [56]. In support of a combined biopsy protocol, differences in the antimicrobial susceptibility profiles of H. pylori isolated from the corpus compared with the antrum have been reported [57,58]. Thus, sampling from both sites avoids resistant H. pylori being missed by the collection of only a single sample from one site of the stomach [6]. To prevent contact with air and desiccation, biopsy specimens for culture should be transported in leak-proof containers containing a dedicated transport medium (e.g. Portagerm pylori, bioMérieux, Marcy-L’Etoile, France). Biopsies should be processed for culture as early as possible following endoscopy, ideally within 6 h [59]. Storage at 4°C is advised if the processing is delayed [55,59]. Biopsy specimens should be inoculated onto Columbia blood agar plates and incubated under microaerobic conditions at 35–37 °C for 7–10 days [60]. The growth medium can be supplemented with antimicrobials (e.g. Helicobacter pylori selective supplement/DENT, Oxoid, Basingstoke, UK) to limit overgrowth with contaminating bacteria or fungi [60,61]. Following culture, the presence of H. pylori should be confirmed by a negative Gram stain and positive oxidase, urease and catalase tests [52]. Current identification systems also include matrix-assisted laser desorption ionisation time-of-flight (Maldi-tof) technology where available [6]. Biopsy specimens taken for culture can also be reused for DNA isolation and detection of H. pylori and resistance-associated mutations by molecular methods
(see statement 6)
.
Statement 6: antimicrobial susceptibility testing by culture or a locally validated molecular method should be performed for national resistance surveillance and before prescribing clarithromycin-containing first-line therapy
Recommendation: strong; quality of evidence: moderate. Resistance to many of the antimicrobials used to treat H. pylori has been increasing over time, and there are geographical variations in resistance patterns [62–64], which are influenced by previous antibiotic exposure in each region [60,62,63]. With respect to antimicrobial stewardship, resistance surveillance is recommended to determine the most appropriate H. pylori eradication regimens in a given population. In addition, European guidelines recommend avoiding the use of first-line clarithromycin triple therapy without prior AST in areas with high or unknown clarithromycin resistance [3] (see statement 9). Culture-based methods are considered the gold standard for H. pylori AST and provide the opportunity to
determine susceptibility to all classes of antimicrobials used to treat H. pylori [65]. Disc diffusion criteria have not been defined for H. pylori, and a minimum inhibitory concentration (MIC) method should be used. For this purpose, the European Helicobacter and Microbiota study group recommends ETEST strips (bioMérieux), which are plastic strips calibrated with a predefined concentration gradient of each antimicrobial [62,65]. Clinical MIC breakpoints for H. pylori antimicrobial resistance are provided by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) and are regularly updated. The most up-to-date MIC resistance breakpoints are as follows: >0.125 mg/L for amoxicillin, >1 mg/L for levofloxacin, >0.25 mg/L for clarithromycin, >1 mg/L for tetracycline, >1 mg/L for rifampicin and >8 mg/L for metronidazole (EUCAST, Clinical Breakpoint Tables Version 14.0, valid from 1 January 2024) [66]. Molecular-based methods for AST eliminate the need for H. pylori culture, as they enable the detection of H. pylori and resistance-associated DNA mutations directly from biopsy material [67,68]. These methods provide a speedier diagnostic option than culture (same day versus 7–10 days, respectively), with less stringent sample storage and transport requirements. Further, the sensitivity of molecular methods is less affected by low bacterial load due to PPI use [49–51,69,70] and studies have shown that the presence of mutations detected by molecular tests correlates well with culture-based susceptibility testing [52,71–73]. A recent study describing multicentre, open-label, randomised, controlled, noninferiority trials demonstrated that the eradication rate using molecular-guided therapy was similar to culture-guided therapy, providing a rationale for the use of molecular-guided treatment in clinical practise [74]. Characterisation of the main DNA mutations associated with clarithromycin and levofloxacin resistance has led to the development of commercially available PCR-based AST kits approved for clinical use. Examples include the ClariRes real time PCR assay (Ingentix, Vienna Austria), the Allplex H.pylori and ClariR assay (Seegene, Eschborn, Germany), the Ridagene H. pylori assay (R-Biopharm, Darmstadt, Germany) and the Amplidiag H. pylori+ ClariR assay (Mobidiag,Paris, France) for clarithromycin resistance detection, and the GenoType HelicoDR assay (Hain Lifescience, Nehren,Germany) for the detection of both clarithromycin and levofloxacin resistance. Incorporation of such PCR-based assays into routine clinical practise in Ireland now seems more
achievable, since most hospitals have the equipment and skillset to perform PCR-based assays following the COVID-19 pandemic [62,70]. Subject to local validation, molecular methods should be considered as an important approach for monitoring the prevalence of H. pylori antimicrobial resistance nationally, as well as a means for determining whether first-line clarithromycin therapy can be prescribed.
Statement 7: posteradication treatment testing must be performed. If gastroscopy is not required, a urea breath test is recommended for posteradication treatment testing. If the urea breath test is unavailable, the monoclonal stool antigen test is an alternative if locally validated
Recommendation: strong; quality of evidence: high. In line with Maastricht VI guidelines, testing for H.pylori eradication should be performed at least 4–6 weeks following the completion of any therapy for H. pylori [3,6]. This period of time is required to exclude the possibility of bacterial suppression leading to false negative results [3]. The UBT is recommended for posteradication testing where available. The monoclonal stool antigen test is an alternative (see statement 2). As antibodies to H. pylori persist for months following infection, serology is not recommended for eradication confirmation. If endoscopy is performed, biopsy sampling should be performed as described in statements 3–5.
Statement 8: proton pump inhibitors significantly reduce the accuracy of the recommended H. pylori tests; therefore, proton pump inhibitors should be stopped 14 days before testing unless PCR testing is available
Recommendation: strong; quality of evidence: high. PPIs should be avoided 2 weeks before diagnostic testing by the UBT, stool antigen test, histology, the RUT or culture [3] as they decrease the bacterial load [27,28,60,75], thus increasing the risk of false negative results [75–78]. However, the working group notes that as PPIs are now available over the counter, many patients do not avoid PPIs before H. pylori testing. As it is less affected by PPI use, PCR is a diagnostic option that overcomes this problem but may not always be available. H2 receptor antagonists may slightly decrease bacterial load, but their use is not considered a problem during H.pylori diagnosis [3,28,79]. Antimicrobials and bismuth should be avoided for 4 weeks before testing [3] as these agents also suppress infection and reduce test sensitivity [27,28].
Domain 2: first-line treatment of Helicobacter pylori infection
Statement 9: 14-day clarithromycin-based triple therapy with a high-dose proton pump inhibitor can only be recommended in cases where clarithromycin susceptibility has been confirmed
Recommendation: strong; quality of evidence: moderate. Since the publication of the IHPWG guidelines in 2017, clarithromycin-resistant H. pylori has been listed on the WHO priority list of antibiotic-resistant bacteria [80]. A 2018 meta-analysis of 178 studies from 65 countries involving >66,000 H. pylori isolates revealed that primary resistance to clarithromycin is now >15% in all WHO
regions except the Americas and Southeast Asia [64]. This same study demonstrated that clarithromycin resistance is significantly associated with the failure of clarithromycincontaining regimens [64]. Subsequent pan-European resistance studies have also reported high average pri
mary clarithromycin resistance rates ranging from 21.3 to 25.0% [62,81]. Our recent data indicates that primary clarithromycin resistance in Ireland is >25% [62,82]. Cumulative data acquired at both the individual patient level and population-based analyses have linked previous exposure to macrolides with clarithromycin resistance in H. pylori [60,63,81,83,84]. The aim of any antimicrobial therapy is to reliably cure H. pylori infection in ≥90% of patients [3,85]. A recent network analysis of the effectiveness of multiple first-line treatments worldwide demonstrated that standard triple therapy was the least efficacious regimen analysed [86]. An audit of first-line clarithromycin triple
therapy from Tallaght University Hospital over a 3-year period (2019–2021) revealed a suboptimal eradication rate of 82.5% (N = 227/275) [87]. As first-line clarithromycin triple therapy should not be used empirically in areas where clarithromycin resistance is known to be >15% [3,28,88], and local eradication rates fall below the 90% target, clarithromycin AST, either by culture or molecular methods (see statements 5 and 6) is recommended before prescribing any clarithromycincontaining therapy [3]. Only in cases where clarithromycin susceptibility is confirmed should clarithromycin-based triple therapy (Table 3 and Fig. 1) be prescribed. The European Registry on the Management of H. pylori infection (Hp-EuReg) has demonstrated that longer treatment durations and higher dose PPI are associated with increased eradication rates in their analysisof first-line treatment outcomes in 21 533 patients over a 5-year period (2013–2018) [89]. Thus, high-dose PPI and treatment durations of 14 days are recommended. While recent studies have demonstrated the potential of the potassium-competitive acid blocker vonoprazan for
acid suppression and enhancing H. pylori eradication rates [86,90–97], vonoprazan is currently not available in Ireland.
|
Table 3.
Recommended treatment descriptions
|
|
Treatment regimen Description Duration
|
|
Clarithromycin PPl
a
b.i.d. 14 days 500 mg clarithromycin b.i.d
amoxicillin 1g amoxicillin b.i.d
triple therapy |
b.i.d., twice daily; PPI, proton pump inhibitor; t.i.d., three times daily; q.i.d., four times daily.
a
Newer generation PPIs such as esomeprazole (40 mg b.i.d.) are recommended.
b
In cases where tetracycline cannot be obtained, 100 mg doxycycline b.i.d. may be used.
Statement 10: bismuth quadruple therapy with a high-dose proton pump inhibitor, metronidazole and tetracycline for 14 days is the recommended first-line treatment in the absence of clarithromycin susceptibility testing or where clarithromycin resistance has been confirmed. Although inferior eradication rates have been reported, doxycycline may be used if tetracycline is
unavailable
Recommendation: strong; quality of evidence: moderate. If primary clarithromycin resistance is >15% and AST is not available before the prescription of first-line therapy, European guidelines [3] recommend bismuth quadruple therapy [PPI, bismuth salt, metronidazole and tetracycline (Table 3)] as the first-line treatment (Fig. 1). Bismuth salts exhibit anti-H. pylori activity in vitro and no resistance to bismuth has yet been reported [98]. Bismuth quadruple therapy containing metronidazole and tetracycline has been shown to consistently achieve first-line cure rates of
>90% in studies published by Hp-EuReg when prescribed independently or in the 3-in-1 capsule [89,99]. Current Irish Health Service Executive guidelines recommend doxycycline rather than tetracycline in bismuth quadruple therapy [100], as doxycycline is less costly and easier to access. It should be noted that lower eradication rates have been reported when doxycycline is given instead of tetracycline in bismuth quadruple therapy [89,101–103]. The treatment duration of bismuth quadruple therapy should be 14 days unless locally validated and equally effective 10-day therapies are available [3]. The European guidelines suggest that nonbismuth quadruple concomitant therapy (PPI, clarithromycin, metronidazole and amoxicillin) may be considered as analternative to bismuth quadruple therapy in areas where dual clarithromycin and metronidazole resistance is below 15% [3,28]. However, this is no longer the case in Ireland (primary dual clarithromycin and metronidazole resistance: 20.6% (N = 26/115)) [82]. In relation to bismuth salts, the options include
De-Noltab (bismuth subcitrate potassium 120 mg) and the 3-in-1 capsule Pylera (140 mg bismuth subcitrate potassium, 125 mg metronidazole and 125 mg tetracycline hydrochloride). De-Noltab is licensed and marketed in the UK but is not licensed in Ireland, where it is considered an Exempt Medicinal Product (EMP). As such, it needs to be sourced by pharmacists through a special wholesaler. De-Noltab is included on the Irish Health Service Executive list of EMPs that may be reimbursed for patients under the general medical services scheme or the drugs payment scheme. Pylera is licensed but not marketed in Ireland, making it currently very difficult for pharmacies to obtain.
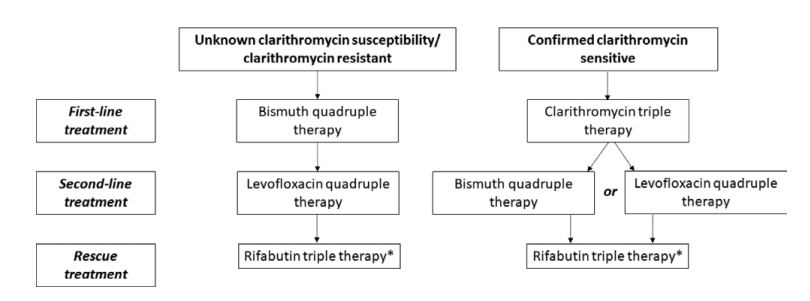
Fig. 1.
Treatment decision schematic. Bismuth quadruple therapy (PPI, bismuth, metronidazole and tetracycline/doxycycline if tetracycline is unavailable); Clarithromycin triple therapy (PPI, clarithromycin and amoxicillin); Levofloxacin quadruple therapy (PPI, bismuth, levofloxacin and amoxicillin); Rifabutin triple therapy (PPI, rifabutin and amoxicillin). *Other rescue therapy options include a PPI and bismuth in combination with two antimicrobials not previously prescribed. PPI, proton pump inhibitor.
Domain 3: second-line and rescue therapy for Helicobacter pylori infection
Statement 11: bismuth quadruple therapy with a high-dose proton pump inhibitor, levofloxacin and amoxicillin for 14 days is the recommended second-line treatment. For those who received antimicrobial susceptibility testing-guided clarithromycin first-line therapy, a combination of proton pump inhibitor, bismuth, metronidazole and tetracycline can be given
Recommendation: strong; quality of evidence: low. Results from recent systematic reviews and meta-analyses have shown no benefit of tailored over empirical second-line and rescue therapy and a failure to reliably achieve cure rates >90% [99,104–106]. The current European recommendations are that empirical second-line and rescue therapy for H. pylori are guided by local resistance surveillance programs and by regularly auditing eradication rates [3]. Primary levofloxacin resistance in Europe is now in the region of 15.8% [62] and is 18.3% (N = 21/115) locally [82]. A local audit from Tallaght University Hospital has shown that the eradication rate for second-line levofloxacin amoxicillin triple therapy was just 68.6%, albeit with a small sample size (N = 35/51; unpublished findings). Data from the Hp-EuReg showed second-line eradication rates increased from 81 to 88% when bismuth was added to levofloxacin amoxicillin triple therapy [107]. Further, the current European Guidelines recommend levofloxacin quadruple therapy (PPI, levofloxacin, amoxicillin and bismuth) as the second line in areas with high clarithromycin resistance [3]. Thus, levofloxacin quadruple therapy (Table 3) is the recommended second-line therapy (Fig. 1). For those who received AST-guided clarithromycin firstline therapy, a combination of PPI, bismuth, metronidazole and tetracycline can be given. The European Medicines Agency has recommended restricted use of fluoroquinolones to infections where the therapeutic benefit outweighs the risk due to rare but serious side effects [3]. Therefore, the use of fluoroquinolones in H. pylori treatment regimens should be restricted to second-line and rescue therapies.
Statement 12: 14-day rifabutin, amoxicillin triple therapy with high-dose proton pump inhibitor is the recommended rescue therapy. Alternatively, a combination of high-dose proton pump inhibitor and bismuth with two antibiotics not previously prescribed can be used
Recommendation: strong; quality of evidence: low. Current European Guidelines recommend empiricalrifabutin triple therapy (Table 3) as the rescue therapy for H. pylori [3]. Irish data on the efficacy of rifabutin-based rescue therapy are lacking but primary resistance is below
10% in Ireland [82], as well as in Europe overall [62]. Although rifabutin has been associated with myelotoxicity, this adverse event is rare and reversible [2]. Data from the Hp-EuReg support the use of rifabutin-based triple therapy as an effective and well-tolerated strategy following one or several failures of H. pylori eradication therapy [108]. The widespread use of rifabutin should be avoided
to prevent resistance selection pressure on Mycobacterium tuberculosis. We, therefore, recommend reserving rifabutin use for third-line and subsequent H. pylori eradication attempts (Fig. 1). As an alternative to rifabutin triple therapy, a combination of high-dose PPI and bismuth with two antibiotics not previously prescribed for 14 days may be used for rescue therapy.
Statement 13: for those with persistent Helicobacter pylori infection following unsuccessful eradication attempts, there is no current evidence-based guideline on appropriate follow-up. The IHPWG consensus is that endoscopic surveillance with ESGE-recommended mapping biopsies for precancerous changes should be considered at an interval of 5-10 years from last failed treatment
Recommendation: strong; quality of evidence: low. Mainly due to poor patient compliance and the increasing prevalence of antimicrobial resistance, H. pylori treatment failure has become more common leading to challenges in H. pylori management [109]. Over decades, H. pylori gastritis may progress through a cascade of precancerous stages from intestinal metaplasia, followed by dysplasia and finally carcinoma [110,111]. Evidence-based recommendations on the management of persistent H. pylori infection following multiple eradication attempts are lacking. While biomarkers for precancerous changes are under investigation, none can currently be recommended for routine clinical use. The IHPWG consensus recommends endoscopic surveillance with the European Society for Gastrointestinal Endoscopy/ management of epithelial precancerous conditions and lesions in the stomach mapping biopsies for precancerous changes [112] at an interval of 5–10 years from the last failed H. pylori eradication attempt to monitor for signs of mucosal progression. In addition, the development of new symptoms at any stage during follow-up, especially any alarm symptoms, should trigger further assessment. Finally, the persistence of H. pylori infection should be considered as a relevant factor by any clinician prescribing nonsteroidal
anti-inflammatory drugs or long-term PPIs.
Statement 14: as part of a quality assurance programme, Helicobacter pylori first-line, second-line and rescue therapy eradication rates should be locally monitored and audited as part of national and European registries
Recommendation: strong; quality of evidence: moderate. There are geographical variations in the prevalence of H. pylori antimicrobial resistance [62–64] and resistance is a continuously evolving process. Therefore, resistance surveillance is recommended (see statement 6). Currently, there is no national program for longterm resistance surveillance in Ireland. Monitoring the eradication success to the various treatment regimens prescribed offers an additional and more widely accessible approach to select the most appropriate H. pylori therapies in each population. The IHPWG consensus is that practitioners should perform regular audits of H. pylori treatment outcomes and that the data should be shared by means of a national registry, as well as with the Hp-EuReg, to refine the best-practice recommendations for the management of H. pylori infection in Ireland over time.
Concluding remarks
These consensus recommendations are intended to provide the most relevant current best-practice guidelines for the management of H. pylori infection in adult patients in Ireland, with a view to improving eradication rates and preventing the progression of H. pylori-associated disease.
As antibiotic resistance is a constantly evolving process, an on-going effort to monitor both antibiotic resistance rates and eradication rates should be made at a national level with centralised data collection protocols.
Acknowledgements
This work was supported by a Health Research Board Applied Partnership Award (HRB-APA-2019-030) and a Health Research Board Investigator-led Project (HRB-ILP-POR-2022-048).-
Conflicts of interest
There are no conflicts of interest.
References