
Adult Guidelines
Abdomen
Abdomen
- The regimens below may NOT cover Multi-drug Resistant Organisms (MRDO) in all cases. See note on MDRO .
- Fungal Infection is an important consideration in patients with intra-abdominal sepsis. In patients at high risk of fungal infection e.g. upper GI perforation, consider antifungal therapy; discuss with Microbiology.
- Most patients with acute pancreatitis do NOT have necrotising pancreatitis and do NOT require antibiotic prophylaxis.
|
Empiric Antibiotics for Abdominal Infections |
||||||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
||
|
See penicillin hypersensitivity section for further information |
||||||
|
The regimens below may NOT cover Multi-drug Resistant Organisms (MRDO) in all cases. See note on MDRO |
||||||
|
Intra-abdominal Mild Community Acquired e.g. cholecystitis/ appendicitis/ diverticulitis |
Co-amoxiclav IV 1.2g every 8 hours |
CefUROXime IV 1.5g every 8 hours + Metronidazole IV 500mg every 8 hours |
Ciprofloxacin IV 400mg every 12 hours + Metronidazole IV 500mg every 8 hours |
Duration 4 to 7 days assuming adequate source control |
||
|
Intra-abdominal Moderate to Severe Community & All Hospital Acquired including cholangitis/ intra-abdominal abscess/diverticulitis |
Piperacillin/ tazobactam IV 4.5g every 8 hours Add Gentamicin IV IF haemo-dynamically unstable. Give one dose per LAPP App calculator. See footnote* re further doses and monitoring. |
CefTRIAXone IV 2g every 24 hours + Metronidazole IV 500mg every 8 hours Add Gentamicin IV IF haemodynamically unstable. Give one dose per LAPP App calculator. See footnote* re further doses and monitoring. |
Ciprofloxacin IV 400mg every 12 hours + Gentamicin IV one dose per LAPP App calculator. See footnote* re further doses and monitoring. + Vancomycin IV infusion, dose per LAPP App calculator. See footnote* re monitoring. + Metronidazole IV 500mg every 8 hours |
Discuss with Microbio-logy. Duration 7 to 10 days assuming adequate source control. |
||
|
Necrotising Pancreatitis Patients with acute pancreatitis admitted to ICU or necrotising pancreatitis confirmed by imaging |
CefTRIAXone IV 2g every 24 hours + Metronidazole IV 500mg every 8 hours |
Ciprofloxacin IV 400mg every 12 hours + Metronidazole IV 500mg every 8 hours |
Review need for antibiotics every 72 hours. See note below. |
|||
|
Discuss with Microbiology if deterioration or requiring antibiotics for more than 5 days |
||||||
|
Spontaneous Bacterial Peritonitis |
CefTRIAXone IV 2g every 24 hours |
Ciprofloxacin IV 400mg every 12 hours |
5 days |
|||
|
Peritoneal Dialysis Peritonitis |
Please see Peritoneal Dialysis in the Renal Dosing Section. |
|||||
|
Cirrhosis with Acute Variceal Haemorrhage, Prophylaxis |
CefTRIAXone IV 2g every 24 hours |
CefTRIAXone IV 2g every 24 hours |
500mg every 12 hours |
7 Days |
||
|
Prophylaxis for patients with an absent or dysfunctional spleen |
Phenoxymethyl-penicillin PO 666mg (Calvepen ® )
every 12 hours
Amoxicillin PO 500mg every 24 hours |
Erythromycin PO 250 to 500mg every 24 hours |
Oral absorption of phenoxymethylpenicillin is limited and affected by a number of variables. For emergency self initiated therapy of a suspected systemic infection treatment with amoxicillin is preferable. See Appendix 3 for guidelines for management of patients with absent or dysfunctional spleen (adults only) including recommended vaccines & antibiotics. |
|||
|
Emergency treatment doses |
||||||
|
Amoxicillin PO 500mg to 1g every 8 hours |
Erythromycin PO 500mg to 1g every 6 hours |
|||||
|
* Review need for ongoing Gentamicin and Vancomycin on a daily basis. Continue with once daily Gentamicin dosing ONLY if C onsultant/Registrar recommended. For advice on monitoring see Aminoglycoside & Vancomycin Dosing & Monitoring section. |
||||||
Refs:
- IDSA Guidelines for Diagnosis and Management of Complicated Intra-abdominal infections in Adults & Children. Clin Infect Dis 2010;50:133-164
- ISPD Peritoneal dialysis-related infections: recommendations 2010 update. Peritoneal Dialysis International July 2010;30:393-423
Bone and Joint
Bone and Joint
- Microbiological diagnosis is essential , relevant bone and synovial fluid samples should be sent prior to treatment. Treatment should be targeted at the infecting organism.
- Discussion with Microbiology is recommended in all cases.
- The regimens below may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. See note on MDRO .
- These guidelines are intended for adults only.
|
Empiric Antibiotics for Bone and Joint Infections |
|||||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
|
|
See penicillin hypersensitivity section for further information |
|||||
|
The regimens below may NOT cover Multi-drug Resistant Organisms (MRDO) in all cases. See note on MDRO |
|||||
|
Septic Arthritis |
Flucloxacillin IV 2g every 6 hours OR CefTRIAXone IV 2g every 24 hours ( IF high risk of Gram-negative organisms (e.g. elderly; nursing home resident; recurrent UTIs) or risk of gonococcus) |
Vancomycin IV infusion, dose per LAPP App calculator. See footnote* re monitoring. OR CefTRIAXone IV 2g every 24 hours ( IF high risk of Gram-negative organisms (e.g. elderly; nursing home resident; recurrent UTIs) or risk of gonococcus) |
Discuss with Microbiology |
Adequate drainage of joint fluid essential. Blood cultures also required. Gram stain may alter antibiotic therapy. Minimum 2 weeks parenteral therapy. Discuss with Microbiology. |
|
|
Osteomyelitis |
Discuss with Microbiology; treat according to culture results. |
||||
|
Prosthetic Joint Infection |
Discuss with Microbiology; treat according to culture results. |
||||
|
*For advice on monitoring see Vancomycin Dosing & Monitoring section. |
|||||
Ref:
- BSR & BHPR, BOA, RCGP and BSAC guidelines for management of the hot swollen joint in adults Rheumatology 2006;45:1039-1041
Cardiovascular
Bacterial Endocarditis
Bacterial Endocarditis
- The following is intended primarily to provide initial short-term guidance on empiric therapy of seriously ill patients and those with prosthetic valves.
- Immediate discussion on the next day with Microbiology is recommended in all cases of suspected endocarditis.
- In those with sub-acute presentation of suspected endocarditis, with a native valve and who are clinically stable at presentation it is often preferable to send blood cultures (as below) and to withhold antibiotics pending consultation and culture results.
- In all but the most profoundly ill patients take 3 sets of blood cultures (10ml into each of two bottles for each set) BEFORE any antibiotics are given. If the patient is seriously ill the interval between cultures can be as short as 20 or 30 minutes.
- For full detailed guidance on management see the European Society of Cardiology Guidelines for Management of Endocarditis 2023 or click here to download the ESC Pocket guidelines app to your phone.
|
Empiric Antibiotics for Bacterial Endocarditis |
||||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
|
See penicillin hypersensitivity section for further information |
||||
|
Bacterial Endocarditis Community Acquired Native Valve Endocarditis or late Prosthetic Valve Endocarditis ( ≥ 12 months post-surgery) |
Amoxicillin IV 2g 4 hourly + Flucloxacillin IV 2g 4 hourly + Gentamicin IV 3mg/kg/day (maximum 240mg/day). See footnote* re monitoring.
|
CeFAZOLin IV 2g TDS + Gentamicin IV 3mg/kg/day (maximum 240mg/day). See footnote* re monitoring. |
Vancomycin IV infusion, dose per LAPP App calculator . See footnote** re monitoring. + Gentamicin IV 3mg/kg/day (maximum 240mg/day). See footnote* re monitoring. |
Once culture and sensitivity results are available direct antibiotic therapy accordingly in discussion with Microbiology .
Rifampicin PO 450mg every 12 hours can be added for prosthetic valve endocarditis, it may be preferrable to delay this for 3-5 days after commencement of other antibiotic therapy.
Duration as advised by Microbiology.
|
|
Early Prosthetic Valve Endocarditis (<12 months post-surgery), nosocomial or non-nosocomial healthcare-associated Infective Endocarditis
|
Vancomycin IV infusion, dose per LAPP App calculator . See footnote** re monitoring. +
Gentamicin IV 3mg/kg/day (maximum 240mg/day)
+ Rifampicin PO 450mg 12hrly 1 [Can be given IV if PO route not available] ( 1 Consider delaying initiation of Rifampicin for 3 to 5 days after commencement of Vancomycin and Gentamicin, once the bacteraemia has been cleared).
|
|||
|
* For advice on monitoring of Gentamicin for the treatment of Infective Endocarditis see the Aminoglycoside Dosing & Monitoring section (table 4 - Once daily low dose Gentamicin in Infective Endocarditis) ** Review need for ongoing Vancomycin on a daily basis. For advice on monitoring see Vancomycin Dosing & Monitoring section. |
||||
References:
- Gould et al. BSAC Guidelines for the diagnosis and antibiotic treatment of endocarditis in adults. Journal of Antimicrobial Chemotherapy 2012;67:269-289
- Baddour et al. AHA Infective Endocarditis: Diagnosis, Antimicrobial Therapy, and Management of Complications. Circulation 2015;132:1435-1486
- Habib et al. ESC Guidelines on the prevention, diagnosis & treatment of infective endocarditis. European Heart Journal 2015;36:3075-3128
- Delgado et al. ESC Guidelines for the management of endocarditis: Developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM). European Heart Journal , 2023 ; 44: 3948–40
Prophylaxis of Infective Endocarditis
Prophylaxis of Infective Endocarditis
- The routine use of antibiotics in most situations is NOT justified on the balance of risk and benefit.
- Discussion with Microbiology recommended if infection at procedure site.
- Only patients identified with the following cardiac conditions undergoing one of the following high risk procedures should be considered for prophylaxis for infective endocarditis (IE):
|
Prophylaxis of Infective Endocarditis |
||
|
Box 1: Cardiac conditions requiring endocarditis prophylaxis - for high risk procedures |
||
|
||
|
Box 2: Recommendations by procedure - for patients with identified cardiac conditions |
||
|
A. Dental Procedures Antibiotic prophylaxis should only be considered for dental procedures requiring manipulation of gingival or periapical region of teeth or perforation of oral mucosa. Antibiotic prophylaxis is not recommended for local anaesthetic injections in non-infected tissue, removal of sutures, dental X-rays, placement or adjustment of removable prosthodontic or orthodontic appliances or braces, or following shedding of deciduous teeth, or trauma to lips or oral mucosa. |
||
|
B. Respiratory Tract Procedures Antibiotic prophylaxis should only be considered for invasive procedures involving incision or biopsy of the respiratory mucosa e.g. tonsillectomy or adenoidectomy, or to treat infection e.g. drainage of abscess or empyema. Antibiotic prophylaxis is not recommended for respiratory tract procedures, including bronchoscopy or laryngoscopy, transnasal or endotracheal intubation. |
||
|
C. Gastrointestinal or genitourinary tract procedures Antibiotic prophylaxis is not recommended for any procedure. |
||
|
Box 3: Recommended prophylaxis for procedures at risk |
||
|
Give as a single dose 30 to 60 minutes before procedure |
||
|
Procedure |
1st line antibiotic |
Alternative if penicillin allergic |
|
Dental |
Adults: Amoxicillin PO/IV 2g
|
Adults: Doxycycline 100mg PO
|
|
Respiratory |
As for dental |
|
References:
- Wilson et al. AHA Guideline Prevention of Infective Endocarditis. Circulation 2007;116:1736
- Habib et al. ESC Guidelines on the prevention, diagnosis & treatment of infective endocarditis. European Heart Journal 2015;36:3075-3128
- Delgado et al. ESC Guidelines for the management of endocarditis: Developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM). European Heart Journal , 2023 ; 44: 3948
Central Nervous System
Suspected Bacterial Meningitis
Suspected Bacterial Meningitis
- The most important aspect of treatment of suspected or confirmed bacterial meningitis is to commence antibacterial therapy IMMEDIATELY .
- IV Chloramphenicol is available in the Emergency Department and in the Pharmacy Department (unlicensed room). Meropenem may be an alternative to chloramphenicol in patients with a history of penicillin anaphylaxis, as recommended in Irish guidelines, with close monitoring for cross-sensitivity. Please discuss with Microbiology.
- See footnote on use of Dexamethasone.
- Discuss with Microbiology - essential if risk factors for M. tuberculosis (alcohol, homelessness, immunocompromised host, recent immigration from area of high incidence, recent contact with tuberculosis) or if history of neurosurgery, head trauma or if device-related infection e.g. central nervous system shunt, ventricular drain or other.
- Risk factors for Listeria monocytogenes meningitis in adults include patients who are immunocompromised, have chronic illness such as alcohol dependency, diabetes, and malignancy or age over 60.
- Viral meningitis (as distinct from encephalitis) generally does NOT require anti-viral treatment. Discuss with Microbiology.
- See Appendix 4 for management of contacts.
|
Empiric Antibiotics for Suspected Bacterial Meningitis |
||||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
|
See penicillin hypersensitivity section for further information |
||||
|
Suspected Bacterial Meningitis |
CefTRIAXone IV 2g every 12 hours + Consider adding Amoxicillin IV 2g every 4 hours if at risk for L. monocytogenes (See point 5 above)
See footnote ** re Dexamethasone. |
CefTRIAXone IV 2g every 12 hours + Consider adding Co-trimoxazole IV 60mg/kg every 12 hours (round dose to nearest multiple of 480mg) if at risk for L. monocytogenes (See point 5 above)
See footnote ** re Dexamethasone. |
Chloramphenicol IV 25mg/kg
Consider adding Co-trimoxazole IV 60mg/kg every 12 hours (round dose to nearest multiple of 480mg) if at risk for L. monocytogenes Discuss need for nasopharyngeal eradication for the patient with Microbiology (See point 5 above)
See footnote ** re Dexamethasone. |
Minimum duration of treatment: Meningococcal meningitis: 5 to 7 days
Haemophilus meningitis: 7 to 10 days
Pneumococcal meningitis: 10 to 14 days
Listeria meningitis: 21 days |
|
|
If patient has, within the last 6 months, been to a country where penicillin resistant pneumococci are prevalent , IV Vancomycin should be added , dose per LAPP App calculator. See footnote* re review and monitoring. Recommend discussion with Microbiology. Note: Up to date European and worldwide data on resistance can be found via the European Centre for Disease Prevention and Control website . Or please consider a discussion with Microbiology if recent travel. |
|||
|
* Review need for ongoing vancomycin on a daily basis. For advice on monitoring see Vancomycin Dosing & Monitoring section. |
||||
|
**Dexamethasone
|
||||
References:
- NICE guideline NG240 . Meningitis (bacterial) and meningococcal disease: recognition, diagnosis and management. Published 19 March 2024 [Accessed 19/3/2026]
- HPSC Guidelines for the Early Clinical and Public Health Management of Bacterial Meningitis (including meningococcal disease) November 2016
- Mc Gill at al “The UK Joint specialist societies guidelines on the diagnosis and management of acute meningitis and meningococcal sepsis in immunocompetent adults” British Infection Society 2016
- BNF 86 March 2024
Suspected Herpes Simplex Encephalitis
Suspected Herpes Simplex Encephalitis
- Viral meningitis (as distinct from encephalitis) generally does NOT require anti-viral treatment. Discuss with Microbiology
- Discussion with Microbiology recommended if patient has recent travel history or is immunocompromised.
|
Antivirals for Suspected Herpes Simplex Encephalitis |
||
|
Infection |
1 st Line |
Comment |
|
Suspected Herpes Simplex Encephalitis |
Aciclovir IV 10mg/kg every 8 hours
If obese, consider using ideal or adjusted body weight to calculate dose – See Medinfo GUH IV guideline for more details. |
Confirmed HSV encephalitis requires a total of 14 to 21 days IV therapy. |
Reference
- IDSA Guidelines for the Management of Encephalitis Clin Infect Dis 2008;47:303-27
Conjunctivitis
Acute Bacterial Conjunctivitis
- Acute Conjunctivitis can be divided into bacterial, viral, allergic or non-specific aetiologies. All are self-limiting and often resolve within 5-7 days without treatment . Antimicrobial therapy is of very limited value in most cases of conjunctivitis.
- This guidance is specifically for acute non-gonococcal, non-chlamydia bacterial conjunctivitis . If concerned regarding chlamydia or gonococcal conjunctivitis discuss with Microbiology AND Ophthalmology.
- A red eye is generally a sign of inflammation of the conjunctiva (conjunctivitis). Although conjunctivitis is the most common cause of a red eye there are other benign (dry eye, blepharitis, subconjunctival haemorrhage, episcleritis) and sight threatening (uveitis, sclerits, endophthalmitis, acute glaucoma) causes.
- Any of the following red flag features should trigger a same day referral to Ophthalmology :
- Acute reduction in vision of the affected eye
- Severe pain/photophobia
- Contact lens use
- Recent intraocular surgery
- Recent intravitreal injection
- Prior glaucoma filtration surgery (Trabeculectomy)
- Abnormal pupil shape, unequal pupil size or a pupil that reacts poorly to light
- Copious mucopurulent discharge
- Bacterial conjunctivitis may be associated with mucopurulent discharge, and the lids are often "glued" on waking. Send a swab for culture and sensitivity. Topical chloramphenicol or fusidic acid may be used (see below).
- Note Chloramphenicol is not recommended in pregnancy or breastfeeding.
- Prolonged or recurrent use of any topical agent can lead to the emergence of resistance and should be avoided.
|
Empiric Treatment of Acute Bacterial Conjunctivitis |
||
|
Infection |
Treatment |
Comment |
|
Acute Bacterial Conjunctivitis |
Chloramphenicol 0.5% eye drops — apply 2 drops 3 hourly during waking hours or more frequently if required. Or Chloramphenicol 1% eye ointment (Unlicensed) — apply every 6 hours or apply at night only if used in conjunction with chloramphenicol drops. Or Fusidic acid 1% eye drops — can be used second line. Apply 1 drop every 12 hours. |
Duration 48 hours after resolution of symptoms Note risk of local hypersensitivity reaction to antimicrobial. |
References:
- National Institute for Health and Care Excellence (2017) Conjunctivitis-infective (CKS)Available at https://cks.nice.org.uk/conjunctivitis-infective
- BNF 74 September 2017
- HSE Conjunctivitis - Antibiotic Prescribing Reviewed - October 2022
- Summary of Product Characteristics. Chloromycetin 0.5% w/v Redidrops Eye Drops, Solution - Last updated August 2022
Orbital and Periorbital Cellulitis
Orbital and Periorbital Cellulitis
See Orbital and Periorbital Cellulitis in Skin & Soft Tissue Infections Section
Fungal
Fungal
- Medical assessment is required before prescribing antifungal therapy.
- For suspected oral candidiasis send a swab to microbiology to confirm fungal infection.
- For recurrent or refractory infection send a repeat swab and discuss with Microbiology.
- In immunocompromised patients a high index of suspicion of infection is advised.
|
Empiric Treatment of Fungal Infections |
||
|
Infection |
Treatment |
Comment |
|
Oropharyngeal candidiasis |
Mild Nystatin suspension PO 5ml every 6 hours after food. Swish and swallow, leaving in contact with mouth for at least 30 seconds. |
Duration usually for 7 days, continued for 48 hours after lesions have resolved. |
|
Moderate to severe Fluconazole PO 200mg loading dose on day 1 followed by 100mg every 24 hours |
Duration 7 to 14 days |
|
|
Fluconazole refractory Contact Microbiology |
||
|
Denture related As above plus disinfection of dentures. |
||
|
Oesophageal candidiasis |
Fluconazole PO 400mg loading dose on day 1 followed by 200mg every 24 hours |
Duration 14 to 21 days |
|
Acute Vulvovaginal candidiasis (VVC) |
Recommended regimen:
Clotrimazole 2% cream topically 2-3 times daily for 7-14 days
Add Fluconazole PO 150mg as a single dose if not responding.
Severe Acute VVC: Fluconazole PO 150mg every 72 hours for 3 doses
Acute VVC in Pregnancy and breastfeeding: Clotrimazole pessary 500 mg intravaginally at night for up to 7 consecutive nights
Fluconazole refractory/severe/recurrent PVC Contact Microbiology
|
|
|
Candida at urinary, respiratory & other sites |
Treatment not routinely indicated. Contact Microbiology |
|
|
Disseminated candidiasis |
Contact Microbiology. Choice of antifungal depends on sensitivities. |
|
|
Fungal skin infection |
Contact Microbiology or Dermatology for advice. |
|
|
Fungal nail infection |
Contact Microbiology or Dermatology for advice. |
|
|
For all other suspected fungal infections e.g. aspergillosis contact Microbiology |
Contact Microbiology for advice. |
|
References:
- IDSA Candidiasis Guidelines Clin Infect Dis 2016;62:e1-e50
- BASHH UK National Guideline on the Management of Vulvovaginal Candidiasis 2007
- Centers for Disease Control and Prevention . Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1-137
- IDSA 2016 Clinical Practice Guideline Update for the Management of Candidiasis published December 16, 202
Gastrointestinal System
Clostridioides difficile Infection (CDI)
Clostridioides difficile Infection (CDI)
1. The following guidance applies to the treatment of patients with a clinical diagnosis of CDI and supportive microbiological evidence of CDI.
2. Detection of C. difficile GDH +/- gene alone does not diagnose CDI. Clinical assessment is essential . Asymptomatic colonisation can occur in 20-40% of hospitalised patients and does not require treatment.
3. If CDI is diagnosed please see the table below for treatment of initial episode and first recurrence of CDI.
4. The following regimens may be recommended by Microbiology only :
- Regimen for tapered pulsed oral Vancomycin (see Appendix 2 for more information)
- Regimen for intracolonic Vancomycin (see Appendix 2 for more information)
- Reserve agent recommendation e.g. Fidaxomicin
5. See Appendix 2 for CDI Patient information leaflet and CDI Management Practical Guide Summary .
|
Antibiotics for Clostridium difficile Infection |
||
|
Infection |
1 st Line Antibiotics |
Comment |
|
Non severe CDI Mildly symptomatic patients (positive test result but less than 3 episodes of diarrhoea in 24 hours): |
Discontinue antibiotic therapy with the inciting antibiotic if possible and closely monitor the patient for 48 hours. C. difficile treatment should be initiated if any signs of clinical deterioration are observed. |
General measures advised in the treatment of all patients with CDI:
|
|
Non severe CDI Positive test results and 3 or more episodes of diarrhoea in 24 hours : |
1st line
It can be considered as a treatment option for patients at high risk of recurrence supported by age over 65 years plus the presence of one or more of these additional risk factors: - healthcare associated CDI - prior hospitalisation in the last 3 months - use of concomitant antibiotics - PPI started during/after CDI diagnosis - prior CDI episode - immunocompromised or if severe underlying disease and/or renal insufficiency. |
|
|
Severe CDI Defined by one of the following:
Additional supporting factors, when available are distension of the large intestine, peri-colonic fat stranding or colonic wall thickening at imaging. |
Please discuss with Consultant Microbiologist. Early surgical opinion for all patients with severe CDI. Patients with severe CDI should be managed by a multidisciplinary team to include a clinical microbiologist, gastroenterologist, surgeon and pharmacist as needed.
1st line
Alternative 1 st line treatment option but must have prior approval by Consultant Microbiologist:
It can be considered as a treatment option for patients at high risk of recurrence supported by age over 65 years plus the presence of one or more of these additional risk factors: - healthcare associated CDI - prior hospitalisation in the last 3 months - use of concomitant antibiotics - PPI started during/after CDI diagnosis - prior CDI episode - immunocompromised or if severe underlying disease and/or renal insufficiency. |
|
|
Severe complicated/fulminant CDI Defined by the presence of one of the following attributed to CDI:
|
Please discuss with Consultant Microbiologist.
1 st line Vancomycin^ PO/NG 500mg every 6 hours Plus Metronidazole IV 500mg every 8 hours
2
nd
line
|
|
|
First recurrence of CDI Recurrence is present when CDI recurs within 8 weeks after a previous episode, provided the symptoms from the previous episode resolved after completion of initial treatment.
|
Choice depends on first line treatment. Pulsed Vancomycin^ PO may be an option Or Fidaxomicin* PO 200mg every 12 hours These options must be discussed with a Consultant microbiologist. |
|
|
Second or more recurrence of CDI |
Discuss with a Consultant Microbiologist. |
|
|
*Prescribing notes: Fidaxomicin requires a High Tech prescription on discharge and is not routinely stocked in community pharmacies. Please contact ward and community pharmacy at least 24 hours prior to discharge to arrange supply if required. |
||
|
^Vancomycin: If a person has swallowing difficulties or a nasogastric or PEG tube for enteral administration, vials of vancomycin powder for injection may be used to make an extemporaneous oral solution. See package insert or Appendix 2 . Alternatively contact pharmacy for further advice. Vancomycin capsules are not routinely stocked in community pharmacies. Please contact ward and community pharmacy at least 24 hours prior to discharge to arrange supply if required. |
||
References:
- Health Protection Surveillance Centre. Surveillance, Diagnosis and Management of Clostridium difficile Infection in Ireland June 2014
- V1.0 Clostridioides difficile treatment in hospital setting published on April 28th 2023 - HSE Antimicrobial Resistance & Infection Control (AMRIC). https://www.hse.ie/eng/services/list/2/gp/antibiotic-prescribing/conditions-and-treatments/gastro/clostridium-difficile/
- Bishop et al “Management of Clostridioides difficile infection in adults and challenges in clinical practice: review and comparison of current IDSA/SHEA ESCMID and ASID guidelines.” J Antimicrob Chemother 2023; 78: 21-30
- Clinical Practice Guidelines for the Management of Clostridioides difficile Infection in Adults: 2021 Update by SHEA/IDSA
- European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin Microbiol Infect 2021 Dec:27 Suppl 2:S1-S21. doi: 10.1016/j.cmi.2021.09.038. Epub 2021 Oct 20 .
- National Institute of Clinical Excellence Clostridioides difficile infection: Antimicrobial prescribing 2023 [NG199] Published: 23 July 2021, Last reviewed 11 July 2024
Gastroenteritis
Gastroenteritis
- Avoid antimicrobial agents unless there is clinical evidence of invasive disease or the patient is immunocompromised, in which case please discuss with consultant microbiologist.
- Consider viral causes if vomiting is a prominent symptom or if norovirus is active in the community or hospital.
- Maintain hydration.
- Avoid anti-diarrhoeal agents.
- Send stool sample (include travel history on the form if relevant).
- Antimicrobial treatment for gastroenteritis is generally pathogen directed.
Reference:
IDSA 2017 Treatment guidelines for infectious diarrhoea:
Clin Infect Dis 65:1963, 2017
.
Helicobacter pylori Infection
Helicobacter pylori Infection
- Seek advice from gastroenterologist if 1 st or 2 nd line eradication unsuccessful.
- While choosing a treatment regimen for H. pylori , patients should be asked about previous antibiotic exposure and this information should be incorporated into the decision-making process.
- Please consider medication side effects and interactions, when choosing a triple therapy regime.
- Second-line therapy depends on the first-line therapy and should not be the same treatment.
- Testing for eradication is recommended in all patients treated for H. pylori and should occur at least 6 - 8 weeks following treatment. Please inform the patient and the GP - a H. pylori stool antigen test should be performed 6 - 8 weeks after H. pylori eradication. To increase accuracy, patients must not be on any medication that affects H. pylori detection; these include antibiotics (past 4 weeks), PPIs (past 2 weeks), and bismuth (past 4 weeks). If symptomatic relief is required during this period, H2 receptor antagonists and anti-acid medications are recommended.
- Bismuth is available in Ireland as unlicensed medicines (ULM) – and therefore not routinely stocked in community. Please contact community pharmacy at least 24hrs prior to discharge to arrange supply.
- Newer generation PPIs, e.g. esomeprazole 40mg, are considered more effective than first generation PPIs.
|
Antibiotic regimens for Helicobacter pylori Eradication |
|||||
|
1 st Line Helicobacter pylori eradication |
1 st Line Triple Therapy |
Penicillin allergy |
Comment |
||
|
Alternative 1 st Line Quadruple Therapy if:
|
|||||
|
Amoxicillin PO 1g every 12 hours + Clarithromycin PO 500mg every 12 hours + Esomeprazole PO 40mg every 12 hours |
Metronidazole PO 400mg every 8 hours + Doxycycline PO 100mg every 12 hours + Bismuth 1 ( brands include Gastrodenol ® or DeNoltab ® ) PO 120mg every 6 hours (unlicensed) + Esomeprazole PO 40mg every 12 hours |
Duration: 14 days |
|||
|
2
nd
line Helicobacter pylori eradication
Discuss with gastroenterology |
2 nd Line Triple Therapy |
||||
|
Second-line therapy depends on the first-line therapy and should not be the same treatment.
Please discuss options with gastroenterology.
|
|||||
|
2 nd line Therapy |
Alternative 2 nd line therapy
|
||||
|
NO Penicillin allergy |
Penicillin allergy |
||||
|
Clarithromycin PO 500mg every 12 hours + Metronidazole PO 400mg every 12 hours + Esomeprazole PO 40mg every 12 hours |
Levofloxacin PO 250mg every 12 hours + Amoxicillin PO 1g every 12hours + Esomeprazole PO 40mg every 12 hours
|
Metronidazole PO 400mg every 8 hours + Doxycycline PO 100mg every 12 hours + Bismuth 1 ( brands include Gastrodenol ® or DeNoltab ® ) PO 120mg every 6 hours (unlicensed) + Esomeprazole PO 40mg every 12 hours
|
|||
|
1 Bismuth is available in Ireland as an unlicensed medicine. As it is unlicensed it will not be routinely stocked in community pharmacies. Please contact the community pharmacy at least 24 hours prior to discharge to arrange supply. Whilst inpatient brand of Bismuth stocked is Gastrodenal ®. |
|||||
References:
- Irish H. pylori Working Group European Journal of Gastroenterology & Hepatology: 2017;29(5):552–559
- NICE Guideline Gastro-oesophageal reflux disease and dyspepsia in adults: investigation and management Clinical Guidelines [CG184] Published: 03 September 2014 Last updated October 2018
- BNF online (Accessed Feb 2024) Treatment summary: Helicobacter pylori infection
- HSE.ie, Antibiotic Prescribing, Helicobacter pylori, December 2020 (with minor update November 2023) https://www.hse.ie/eng/services/list/2/gp/antibiotic-prescribing/conditions-and-treatments/gastro/helicobacter-pylori/ (Accessed Feb 2024)
- Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Malfertheiner P, et al. Gut 2022;71:1724–1762. doi:10.1136/gutjnl-2022-327745 Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report (bmj.com)
Genital System
Genital System
Discuss with Microbiology.
|
Empiric Antibiotics for Genital System Infections |
|||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
|
See penicillin hypersensitivity section for further information |
|||
|
Pelvic Inflammatory Disease - Outpatient Treatment Send a full STI screen including Chlamydia & Gonorrhoea |
CefTRIAXone IM 1G single dose + Doxycycline PO 100mg every 12 hours + Metronidazole PO 400mg every 12 hours |
Levofloxacin PO 500mg OD ( see Fluroquinolone warning ) + Metronidazole PO 400mg every 12 hours |
Duration 14 days |
|
Pelvic Inflammatory Disease - Inpatient Treatment Send a full STI screen including Chlamydia & Gonorrhoea |
CefTRIAXone IV 2g every 24 hours + Doxycycline PO 100mg every 12 hours + Metronidazole PO 400mg every 12 hours |
Clindamycin IV 900mg every 8 hours + Gentamicin IV every 24 hours, dose per LAPP App calculator . See footnote* re review and monitoring. Followed by an oral switch to: Doxycycline PO 100mg every 12 hours + Metronidazole PO 400mg every 12 hours
Note: The initial IV regimen does not cover Chlamydia or Gonorrhoea. It is important to send a full STI screen. |
Continue IV treatment for 24 hours after clinical improvement.
Total duration of antibiotic therapy 14 days |
|
Acute Prostatitis/ Epididymo-orchitis If Sexually active |
CefTRIAXone IM 1g single dose (or 2g IV if inpatient) + Doxycycline PO 100mg every 12 hours
Send urethral swabs for Chlamydia & Gonorrhoea if sexually active in past six months & refer to Sexually Transmitted Infection (STI) Clinic. |
Duration of 14 days for oral doxycycline.
Consider mumps as aetiology. |
|
|
Acute Prostatitis/ Epididymo-orchitis If NOT sexually active |
Ciprofloxacin PO 500mg every 12 hours (See Fluoroquinolone warning ) IF patient appears septic treat as suspected bloodstream infection: Add Gentamicin IV one dose per LAPP App calculator. See footnote* re further doses and monitoring. |
Duration 14 to 28 days |
|
|
* Review need for ongoing Gentamicin on a daily basis. Continue with once daily Gentamicin dosing ONLY if Consultant/Registrar recommended. For advice on monitoring see Aminoglycoside Dosing & Monitoring section. |
|||
References:
- BASHH UK National Guideline for the Management of Pelvic Inflammatory Disease ( 2019 Interim Update)
- BASHH UK National Guidelines for the management of Epididymo-orchitis 2019
- The 2016 European Guideline on the management of epididymo-orchitis. International Journal of STD & AIDS 2017, Vol. 28(8) 744–749
- The Sanford Guide to Antimicrobial Therapy Digital Update Feb 26, 2018
Intravascular Line
Intravascular Line
-
Blood cultures
should be taken if the patient appears septic and/or if the patient has a central or peripheral vascular catheter (CVC/PVC) exit site infection indicated by the presence of cellulitis or thrombophlebitis. Two sets of blood cultures should be taken using aseptic technique from all patients with suspected intravascular catheter-related infection.
- For CVCs either through the CVC and peripherally or through different lumens of the CVC if blood cultures cannot be drawn from a peripheral vein.
- If it is a triple or quad lumen CVC please take 3 sets of cultures: one peripherally, and the other two from two different lumens. Please ensure these are clearly labelled.
- If evidence of exit site infection, a swab should be taken from the site.
- All PVCs must be removed promptly when there is clinical evidence of infection.
- Management of a CVC-related infection depends on the type of CVC involved, the infecting organism and the associated complications. Recommend a discussion with Microbiology. If the CVC is removed (always conducted under aseptic technique), the tip of the central line should be sent to the microbiology lab in a universal container for culture and sensitivity testing, cut to 4cm in length following removal.
- If blood cultures are positive, please discuss with Microbiology. Repeat cultures may be required to document clearance of the bacteraemia, this is dependent on the infecting organism.
- Infection at the site of CVC/PVC, with no systemic features of sepsis and with negative blood cultures may be treated as a skin/soft tissue infection. Treatment is as follows:
- Removal of the PVC is essential. Removal of the CVC may be indicated as part of the initial treatment, recommend a discussion with Microbiology.
- Initial therapy should be with Vancomycin IV.
- Review at 48 hours and consider switch to Flucloxacillin or other antibiotic if appropriate, based on culture and sensitivity and MRSA results.
7. An antibiotic lock solution is very occasionally recommended by Microbiology. If indicated, contact Microbiology for protocol.
|
Empiric Antibiotics for Intravascular Line Infections |
||
|
Infection |
1 st Line |
Comment |
|
Central and Peripheral IV Catheter Exit Site Infection See notes above |
Vancomycin IV infusion, dose per LAPP App calculator. See footnote* re monitoring. Review at 48 hours, change to pathogen directed therapy based on culture & sensitivity |
Duration 7 to 10 days |
|
Peripheral Line-related Infection and/or Bacteraemia |
Vancomycin IV infusion, dose per LAPP App calculator. See footnote* re monitoring. Review at 48 hours, change to pathogen directed therapy based on culture & sensitivity |
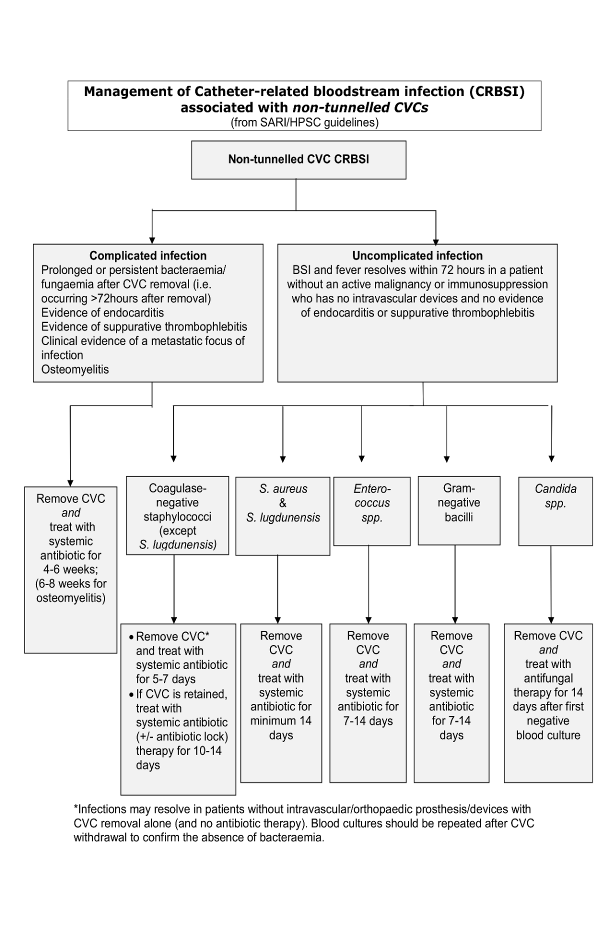
Duration minimum 14 days, for exceptions see algorithm for NON-tunnelled CVC bacteraemia . |
|
Central Line-related Infection and/or Bacteraemia Remove CVC and send tip to microbiology |
Vancomycin IV infusion, dose per LAPP App calculator. See footnote* re monitoring. + Gentamicin IV one dose per LAPP App calculator and review . See footnote* re further doses and monitoring. If blood cultures are positive treat as per Microbiology advice. |
Duration varies by type of line, organism and complications. A prolonged course may be required.
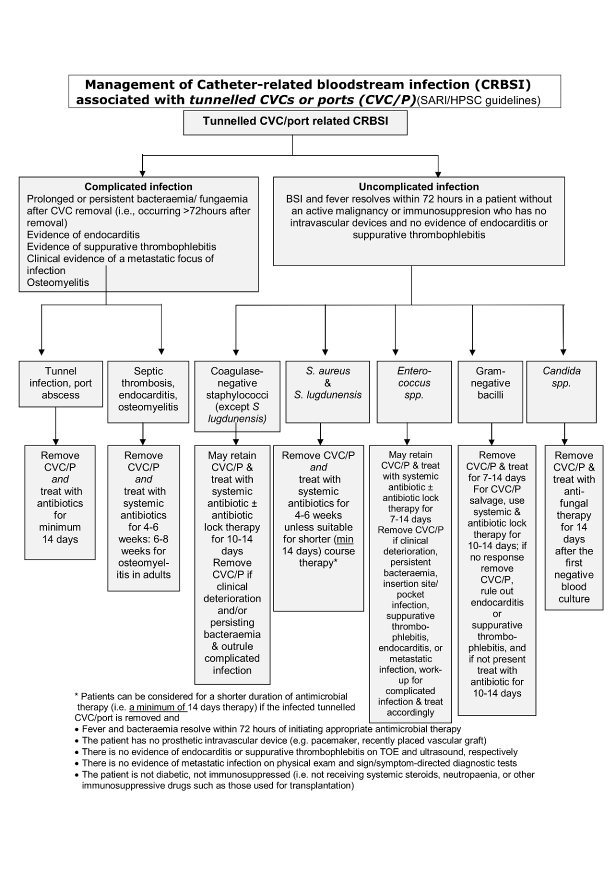
See algorithms for NON-tunnelled CVC bacteraemia and tunnelled CVC/port bacteraemia .
When denoting duration of antimicrobial therapy day 1 is the first day on which negative blood cultures are obtained. |
|
* Review need for ongoing Gentamicin & Vancomycin on a daily basis. Continue with once daily Gentamicin dosing ONLY if Consultant/Registrar recommended. For advice on monitoring see Aminoglycoside & Vancomycin Dosing & Monitoring section. |
||
References:
- HSE/RCPI/HCAI Prevention of Intravascular Catheter-related Infection in Ireland Partial Update of 2009 Guidelines September 2014
- IDSA Guidelines for the diagnosis and management of intravascular catheter-related infection. Clin Infect Dis 2009;49:1-45
Algorithm for Management of NON-tunnelled CVC Bacteraemia
Algorithm for Management of tunnelled CVC/ Port Bacteraemia
Malaria
Malaria
- These guidelines are intended for adults.
- Species of infecting parasite is frequently uncertain
- Discussion with Microbiology recommended.
- Severe malaria is a medical emergency. After rapid clinical assessment, a diagnostic test should be sent. In patients with clinically severe malaria or high parasitaemia (2% or greater) first line treatment is intravenous Artesunate which should be started within one hour of assessment. Intravenous Quinine may be used if Artesunate is unavailable for any reason.
- Follow-on therapy Note for some kinds of malaria additional follow on therapy with Primaquine is required to eradicate the persistent liver stage. All cases must be discussed with Infectious Diseases (GUH) or Microbiology.
- Discharge prescriptions There can be problems with availability and medical card coverage of oral treatment on discharge. Please contact community pharmacy at least 24hours prior to discharge to arrange supply. If there are any issues sourcing please contact inpatient Pharmacy to discuss supply.
- Riamet PO and Artesunate IV are stocked in LUH in the ED Main Omnicell.
|
Malaria Treatment |
|||
|
Indication |
Oral Antimalarials |
Comment |
|
|
1 st Line |
2 nd & 3 rd line |
||
|
Non-severe malaria Non-Pregnant Adult |
Riamet ® PO (over 35kg body weight) 4 tablets PO at 0hrs, 8hrs, 24hrs, 36hrs, 48hrs, 60hours (total 24 tablets over 60 hours) (Four tablets of Riamet ® contain 80mg of Artemether & 480mg of Lumefantrine)
|
Second line: Malarone ® PO 4 tablets every 24 hours for 3 days (Four tablets of Malarone ® contain 1g of Atovaquone & 400mg of Proguanil) OR Third line option - non-pregnant adult only: Quinine PO 600mg (unlicensed) every 8 hours + Doxycycline PO 200mg every 24 hours
Duration 7 days |
Avoid quinine if hypersensitive |
|
Non-severe malaria Pregnant Adult |
All Trimesters: Riamet ® PO (over 35kg body weight) 4 tablets PO at 0hrs, 8hrs, 24hrs, 36hrs, 48hrs, 60hours (total 24 tablets over 60 hours) (Four tablets of Riamet ® contain 80mg of Artemether & 480mg of Lumefantrine) |
Second line: Quinine PO 600mg every 8 hours + Clindamycin PO 450mg every 8 hours
Duration 7 days |
|
|
Severe Malaria Treat as a medical emergency. See notes above. |
Intravenous Antimalarials: If seriously ill or unable to take tablets |
Comment |
|
|
1 st Line |
2 nd line (if artesunate not available). Avoid quinine if hypersensitive. |
||
|
Artesunate IV 2.4mg/kg at 0hrs, 12hrs, 24hours, then every 24 hours until oral treatment can be substituted (see below). |
Quinine IV infusion (Unlicensed) Loading dose*: 20mg/kg (maximum 1.4g) infused over 4 hours, followed 8 hours after start of the loading dose by Maintenance dose: 10mg/kg (maximum 700mg) IV Infusion (over 4 hours) every 8 hours
Reduce maintenance dose to 5 to 7 mg/kg (maximum 700mg) every 8 hours in severe renal impairment, severe hepatic impairment, or if IV treatment continues for more than 48 hours. *Do NOT give loading dose if patient has received quinine or mefloquine in previous 12 hours Oral switch after 24 hours: see below. |
Give intravenous antimalarials in the treatment of severe malaria for a minimum of 24 hours - irrespective of the patient’s ability to tolerate oral medication earlier. Quinine toxicity: ECG monitoring required in the elderly and patients with cardiac disease during IV quinine administration. Significant risk of hypoglycaemia with IV quinine. Monitor blood glucose regularly (about every 2 hours) in the acute situation. |
|
|
A full course of oral treatment should always follow IV artesunate (see below). This applies even if the duration of IV treatment was for 2 days or more. When the patient has had at least 24 hours of IV artesunate (doses at 0hrs, 12hrs, 24 hours) and the patient is able to swallow and absorb medication, give Riamet® PO, starting at least 4 hours after the final dose of IV artesunate. Riamet® PO (over 35kg body weight) 4 tablets at 0hrs, 8hrs, 24hrs, 36hrs, 48hrs, 60 hours (total 24 tablets over 60 hours) (Four tablets of Riamet® contain 80mg of Artemether & 480mg of Lumefantrine)
|
Switch to oral therapy after the first 24 hours (3 doses) to complete a full oral course when the patient is able to swallow AND retain oral medication by giving a course of: Riamet® PO (over 35kg body weight) 4 tablets at 0hrs, 8hrs, 24hrs, 36hrs, 48hrs, 60 hours (total 24 tablets over 60 hours) (Four tablets of Riamet® contain 80mg of Artemether & 480mg of Lumefantrine)
|
||
References:
- WHO Guidelines for the Treatment of Malaria 2023
- Lalloo et al UK malaria treatment guidelines 2016 Journal of Infection 72:635-649
- The Sanford Guide to Antimicrobial Therapy Digital update March 2024
Neutropenic Sepsis
Neutropenic Sepsis
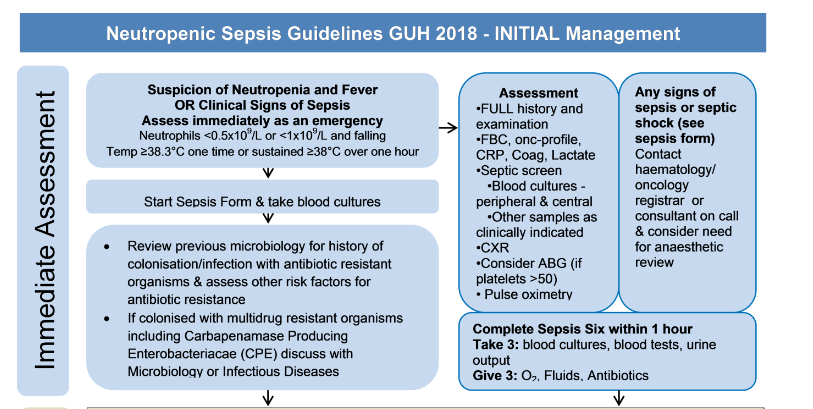
- Any suspicion of neutropenia and fever OR clinical signs of sepsis must be assessed immediately as an emergency.
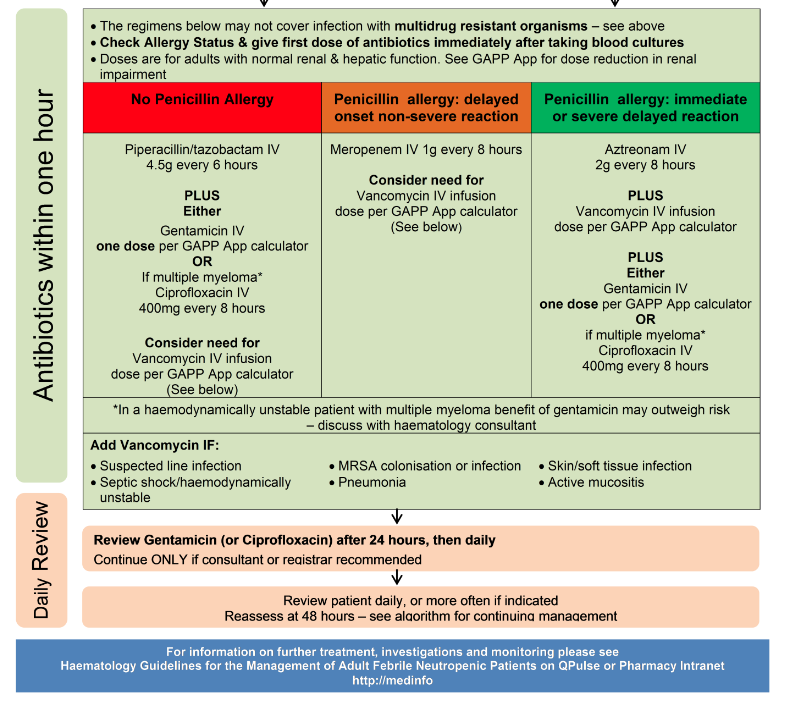
- Antimicrobials must be administered promptly once sepsis is suspected . The HSE sepsis Programme resources and documents are available here.
- Fever means temperature ≥38.0ºC on one or more occasion or sustained.
- Neutropenia means an absolute neutrophil count of less than 0.5 X 10 9 /L or less than 1.0 X 10 9 /L with the possibility of falling further over the next 48 hours.
- Note frequent review is essential . The time frames suggested for addition of additional empiric therapy may need to be shortened if the patient’s condition is deteriorating.
- In addition to the tests recommended in the Immediate Assessment section of the treatment algorithm, please send a sample of urine if clinically appropriate.
- Consider risk for fungal infection and viral infection.
- If the infection is CVC associated - discuss management with the Microbiologist .
- Review previous microbiology for history of colonisation or infection with antibiotic resistant organisms and assess other risk factors for antibiotic resistance. If colonised with Multi-drug Resistant Organisms ( MDRO ) including Carbapenemase Producing Enterobacteriacae (CPE), discuss with Microbiology.
Summary treatment algorithms:
- Initial management of neutropenic sepsis
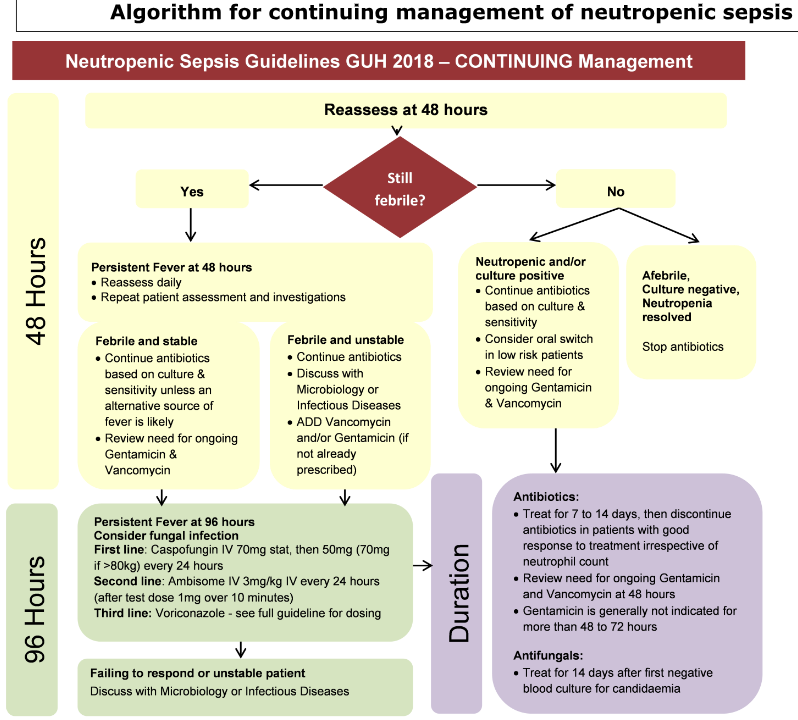
- Continuing management of neutropenic sepsis
References :
- IDSA Guidelines for the use of antimicrobial agents in neutropenic patients with cancer. Clin Infect Dis 2011;52:e56-93
- GUH Haematology Guidelines for the management of febrile neutropenic patients (QPulse CLN-HAEM-020)
- NICE Neutropenic Sepsis: prevention and management in people with cancer ( Clinical guideline 151 ) 2012
- Sepsis 3 Form Adult In-patient Feb 8, 2018
Initial management of neutropenic sepsis - Algorithm
Continuing management of neutropenic sepsis- Algorithm
Obstetrics & Gynaecology
Obstetrics & Gynaecology
**CURRENTLY UNDER REVIEW**
- Discussion with Microbiology recommended for patients showing signs of sepsis.
- Identify need for further intervention to address the source of infection e.g. drainage or removal of source.
- The regimens in the linked documents may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. See note on MDRO .
- Duration of treatment & oral switch is decided on a case-by-case basis depending on subsequent diagnosis as well as clinical progress.
|
Empiric Antibiotics for Obstetric & Gynaecological Infections |
||||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
|
See penicillin hypersensitivity section for further information |
||||
|
The regimens below may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. See note on MDRO |
||||
| National Clinical Programme for Obstetrics and Gynaecology Antimicrobial Prescribing Guidelines for infections including sepsis | https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2018/06/Medication-Guidelines_-Vol-1_Antimicrobial-Prescribing_v1.1-1.pdf | |||
| National Clinical Programme for Obstetrics and Gynaecology Management of UTIs in Pregnancy Guideline | https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2016/05/32.-Management-of-Urinary-Tract-Infections-in-Pregnancy.pdf | |||
| National Clinical Programme for Obstetrics and Gynaecology Preterm Prelabour Rupture of the Membranes (PPROM) Guideline | https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2016/05/19.-Preterm-Prelabour-Rupture-of-Membranes.pdf | |||
| National Clinical Programme for Obstetrics and Gynaecology Chickenpox in Pregnancy Guideline | https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2016/05/35.-Chicken-Pox-in-Pregnancy.pdf | |||
| National Clinical Programme for Obstetrics and Gynaecology Parvovirus B19 Guideline | https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2016/05/26.-Parvovirus-B19-Exposure-Infection-during-Pregnancy.pdf | |||
| National Clinical Programme for Obstetrics and Gynaecology Listeriosis Guideline | https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2016/05/33.-Listeriosis-in-Pregnancy.pdf | |||
| National Clinical Programme for Obstetrics and Gynaecology Antimicrobial Safety in Pregnancy and Lactation Guideline | https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2018/06/Medication-Guidelines_Vol-2_Antimicrobial-safety-in-Pregnancy-and-lactat.._.pdf | |||
|
Chorioamnionitis Discuss considerations around delivery with consultant obstetrician Or Endometritis (Post-partum) If systemically septic follow antibiotic treatment for sepsis |
Co-amoxiclav IV 1.2g every 8 hours + Gentamicin V one dose per GAPP App calculator (use booking weight). See footnote* re further doses and monitoring |
CefTRIAXone IV 2g every 24 hours + Gentamicin V one dose per GAPP App calculator (use booking weight). See footnote* re further doses and monitoring + Metronidazole IV 500mg every 8 hours |
Discuss with Microbiology Ciprofloxacin IV 400mg every 12 hours. See footnote^ re use in pregnancy + Gentamicin IV one dose per LAPP App calculator (use booking weight). See footnote* re further doses and monitoring See footnote^ re use in pregnancy. + Vancomycin IV infusion, dose per LAPP App calculator (use booking weight). See footnote* re monitoring + Metronidazole IV 500mg every 8 hours |
|
|
Preterm Prelabour R upture of Membranes With NO evidence of sepsis/Chorioamnionitis |
Duration 10 days |
|||
|
Erythromycin PO 250mg every 6 hours |
||||
|
Mastitis |
Page 17 of National Clinical Programme for Obstetrics and Gynaecology Antimicrobial Prescribing Guidelines for infections including sepsis https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2018/06/Medication-Guidelines_-Vol-1_Antimicrobial-Prescribing_v1.1-1.pdf |
|||
|
Sepsis |
Page 14 of National Clinical Programme for Obstetrics and Gynaecology Antimicrobial Prescribing Guidelines for infections including sepsis https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2018/06/Medication-Guidelines_-Vol-1_Antimicrobial-Prescribing_v1.1-1.pdf | |||
|
Urinary Tract Infection |
Page 12 of National Clinical Programme for Obstetrics and Gynaecology Antimicrobial Prescribing Guidelines for infections including sepsis https://rcpi-live-cdn.s3.amazonaws.com/wp-content/uploads/2018/06/Medication-Guidelines_-Vol-1_Antimicrobial-Prescribing_v1.1-1.pdf |
|||
|
^Gentamicin & Ciprofloxacin are recommended in pregnancy when benefit outweighs risk. * Gentamicin is generally NOT recommended in pregnancy unless benefit outweighs risk. Review need for ongoing Gentamicin on a daily basis. Continue with once daily Gentamicin dosing ONLY if Consultant/Registrar recommended. For advice on monitoring see Aminoglycoside Dosing & Monitoring section. |
||||
Refs:
- RCOG Bacterial Sepsis in & following Pregnancy, Green-top Guidelines 64a & 64b 2 012
- CDC 2010 Guidelines for the Prevention of Perinatal Group B Streptococcal Disease
- RCOG Group B Streptococcal Disease, early-onset, Green-top Guideline 36 2017
Respiratory System
Antiviral Guidance for Treatment and Prophylaxis of Influenza
Antiviral Guidance for Treatment and Prophylaxis of Influenza
Detailed guidance on the use of antiviral agents for the treatment and prophylaxis of influenza is available on the HSE/HPSC website (please consult).
Antiviral treatment
- Antiviral treatment is recommended as early as possible for any patient with suspected or confirmed influenza who is hospitalised due to influenza.
- Any patient who, while in hospital for another indication, develops influenza, should be assessed for risk from influenza complications (as below). Antiviral treatment is recommended as early as possible for those at higher risk from influenza complications (see table below).
Higher risk from influenza complications includes:
- Age 65 years and over
- Pregnancy (including up to two weeks post-partum)
- Children aged <2 years of age
- Chronic respiratory disease including those on medication for asthma
- Chronic heart, kidney, liver or neurological disease
- Diabetes mellitus
- Haemoglobinopathies
- Immunosuppression (whether due to treatment or disease e.g. HIV)
- Morbid obesity (BMI ≥ 40)
- Those with any condition that can compromise respiratory function (e.g cognitive dysfunction, spinal cord injury, seizure disorder, or other neuromuscular disorder), especially those attending special schools/day centres.
- Those with Down Syndrome
- Persons with moderate to severe neurodevelopmental disorders such as cerebral palsy and intellectual disability
- Residents of nursing homes or Residential Care Facilities.
|
Antiviral regimens for Influenza |
|||
|
Antiviral treatment |
1 st line |
Alternative therapy |
Duration is generally 5 days . There is limited evidence to support treating for longer duration in those with severe influenza (e.g critically ill in ICU) and in severely immunosuppressed patients. Discussion with Microbiology is recommended. |
|
Oseltamivir PO/NG 75mg every 12 hours |
Zanamivir may be indicated for patients if severely immunocompromised – please discuss with Microbiology .
|
||
|
Antiviral prophylaxis |
Chemoprophylaxis (generally PO/NG Oseltamivir) may be considered for people at higher risk from influenza complications (as above, 1 to 13) who have had recent close contact with a person with influenza. Details on use of Oseltamivir for prophylaxis of high risk contacts, including dose and duration are to be found in the HPSC/ HSE guidance . For additional information on renal dosing please see the renal dosing section . |
||
Community Acquired Pneumonia
Community Acquired Pneumonia (CAP)
- CAP is defined as infiltrate on CXR or CT scan with compatible symptoms.
- Give antibiotics as soon as possible, within 4 hours of presentation in the Emergency Department.
- The CURB-65 score, in conjunction with clinical judgement, is a severity assessment tool for Community Acquired Pneumonia. See Clinical Pathway below.
-
Send sputum culture
if severe infection
OR
risk factors for
MRSA
or
Pseudomonas
infection as follows:
- ICU admission
- Hospitalised and/or received IV antibioitcs within past 90 days
- Previous infection with MRSA or Pseudomonas
- Nursing home patients presenting with pneumonia should be treated as CAP as outlined below unless history of Multi-drug Resistant Organisms (MDRO) or recent discharge from hospital.
- Antibiotics are NOT generally recommended for exacerbation of asthma or acute bronchitis with normal CXR - but consider for patients >75years, or those with diabetes, heart failure or immunocompromised.
- Laboratory testing for respiratory viruses should be considered, including COVID-19, and, during relevant season, influenza and Respiratory Syncytial Virus (RSV). Appropriate treatment for COVID-19 or influenza should be initiated if positive or highly suspected due to clinical or epidemiological reasons.
{kind=link}
|
Empiric Antibiotics for Community Acquired Pneumonia (CAP) |
|||||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
|
|
See penicillin hypersensitivity section for further information |
|||||
|
Community Acquired Pneumonia (including nursing home patients unless history of MDRO). See note on MDRO . Signs and symptoms of LRTI AND new consolidation on chest X-ray |
Mild CURB-65 Score 0 or 1 |
||||
|
Amoxicillin PO 1g every 8 hours Consider adding atypical cover with either: Doxycycline PO 100mg every 12 hours Or Clarithromycin PO 500mg every 12 hours |
Doxycycline PO 100mg every 12 hours Or Clarithromycin PO 500mg every 12 hours
|
Duration 5 days (provided afebrile and clinically stable for 48 hours. Otherwise 7 days)
|
|||
|
Moderate CURB-65 Score 2 |
|||||
|
Amoxicillin PO/IV 1g every 8 hours + Add atypical cover with either: Doxycycline PO 100mg every 12 hours Or Clarithromycin PO (IV if NPO) 500mg every 12 hours |
Levofloxacin PO (IV if NPO) 500mg every 12 hours
|
Duration 5 days (provided afebrile and clinically stable for 48 hours. Otherwise 7 days ) Most patients can be treated with oral antibiotics. |
|||
|
Severe CURB-65 Score ≥ 3 |
|||||
|
Co-amoxiclav IV 1.2g every 8 hours + Add atypical cover with either: Doxycycline PO 100mg every 12 hours Or Clarithromycin PO (IV if NPO) 500mg every 12 hours
|
CefTRIAXone IV 2g every 24 hours + Add atypical cover with either: Doxycycline PO 100mg every 12 hours Or Clarithromycin PO (IV if NPO) 500mg every 12 hours |
Levofloxacin PO (IV if NPO) 500mg every 12 hours + Consider adding Vancomycin IV infusion, IF at risk of Staph aureus infection. Dose per LAPP App calculator. See footnote* re review and monitoring. |
Duration 7 days Longer courses are indicated according to clinical judgement and after discussion with Microbiologist e.g. if Legionella pneumophila , Staphylococcus aureus or Gram-negative bacilli suspected or confirmed.
Send urine sample for both pneumococcal and legionella urinary antigen testing in severe CAP. |
||
|
* Review need for ongoing vancomycin on a daily basis. For advice on monitoring see Vancomycin Dosing & Monitoring section. |
|||||
At discharge, refer to GP to ensure COVID-19, influenza and pneumococcal vaccinations are up to date [in eligible populations]. If relevant, provide smoking cessation counselling.
References:
- British Thoracic Society Guidelines for the management of community acquired pneumonia in adults 2009
- American Thoracic Society /Infectious Diseases Society of America Consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44 (suppl 2) S27-72
- Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care 2019;200(7):e45-e67
- Duration of Antibiotic Treatment in Community-Acquired Pneumonia: A Multicenter Randomized Clinical Trial. JAMA Intern Med 2016;176(9):1257-1265
- HSE Immunisation guidance Immunisation - HSE.ie (Accessed 13/02/24)
CAP Clinical Pathway

Aspiration Pneumonia
Aspiration Pneumonia (Community Acquired)
For treatment of aspiration with clinical evidence of pneumonia >5days after hospital admission, refer to Hospital Acquired Pneumonia (HAP) .
Antimicrobial therapy for patients with aspiration without clinical evidence of pneumonia (acute aspiration pneumonitis) does not offer clinical benefit .
|
Empiric Antibiotics for Aspiration Pneumonia |
|||
|
Infection |
1st Line Antibiotics |
In penicillin allergy |
Comment |
|
Aspiration Pneumonia
Note: Antimicrobial therapy for
|
Co-amoxiclav IV 1.2g every 8 hours |
Discuss with Microbiology |
Duration 5 days (provided afebrile and clinically stable for 48 hours. Otherwise 7 days) |
- Dragan et al. Prophylactic Antimicrobial Therapy for Acute Aspiration Pneumonitis. Clin Infect Dis 2018:67(4):513-518
Chronic Obstructive Pulmonary Disease (COPD)
|
Empiric Antibiotics for COPD |
|||
|
Infection |
1st Line Antibiotics |
In penicillin allergy |
Comment |
|
COPD Exacerbation without infiltrate |
Amoxicillin PO 1g every 8 hours
OR
If recent (<2/52) course of amoxicillin:
|
Doxycycline PO 100mg every 12 hours
OR Clarithromycin PO 500mg every 12 hours |
Duration 5 days (provided afebrile and clinically stable for 48 hours. Otherwise 7 days) |
At discharge, refer to GP to ensure COVID-19, influenza and pneumococcal vaccinations are up to date [in eligible populations]. If relevant, provide smoking cessation/medication counselling and ensure patient is on appropriate therapy to enhance control of chronic COPD.
- Infective exacerbation of COPD. HSE Antibiotic prescribing Guidelines for Treatment of Community Infections. Accessed Nov 2023
Hospital Acquired Pneumonia
Hospital Acquired Pneumonia
- Pneumonia should be treated as hospital acquired if onset from 5 days after hospital admission. If recent hospital admission or multiple admissions over the previous 6 to 12 months please discuss with consultant Microbiologist .
- The regimens below may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. See note on MDRO .
- Intensive care and immunosuppressed patients should be discussed with Microbiology.
|
Empiric Antibiotics for Hospital Acquired Pneumonia |
||||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
In penicillin allergy |
Comment |
|
See penicillin hypersensitivity section for further information |
||||
|
The regimens below may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. See note on MDRO |
||||
|
Hospital Acquired Pneumonia Contact Microbiology for treatment of Pseudomonal infection. |
Moderate
Piperacillin/tazobactam IV
|
Moderate
CefTRIAXone IV 2g
Add Gentamicin IV IF haemodynamically unstable. Give one dose per LAPP App calculator. See footnote* re further doses and monitoring.
Note if history of Pseudomonas colonisation/infection discuss alternative treatment with microbiologist. |
Moderate Vancomycin IV infusion, dose per LAPP App calculator. See footnote* re monitoring. +
Ciprofloxacin
** IV
If possible aspiration Add
Metronidazole IV
Add Gentamicin IV IF haemodynamically unstable. Give one dose per LAPP App calculator. See footnote* re further doses and monitoring. |
Duration 7 days May need to be extended according to clinical judgement in discussion with microbiology e.g. if Legionella pneumophila , Staphylococcus aureus or Gram-negative bacilli suspected or confirmed. |
|
|
Severe (ICU assessment required) Piperacillin/tazobactam IV 4.5g every 6 hours + Vancomycin IV infusion, dose per LAPP App calculator. See footnote* re review and monitoring. Review at 24 - 48 hours and stop if MRSA not detected from clinical samples or MRSA screen. Add Gentamicin IV IF haemodynamically unstable. Give one dose per LAPP App calculator. See footnote* re further doses and monitoring |
Severe (ICU assessment required) Vancomycin IV infusion, dose per LAPP App calculator. See footnote* re monitoring. +
Ciprofloxacin
** IV
If possible aspiration add
Metronidazole IV
Add Gentamicin IV IF haemodynamically unstable. Give one dose per LAPP App calculator. See footnote* re further doses and monitoring. |
||
|
* Review need for ongoing Gentamicin and Vancomycin on a daily basis. Continue with once daily Gentamicin dosing ONLY if recommended by the patient's Consultant/Registrar . For advice on monitoring see Aminoglycoside & Vancomycin Dosing & Monitoring section. **Switch from IV to oral Ciprofloxacin (500mg PO every 12 hours) as soon as possible. |
||||
References:
- American Thoracic Society/Infectious Diseases Society of America. Management of adults with hospital-acquired and ventilator-associated pneumonia Clin Infect Dis 2016;63:e61-111
- BSAC Guidelines for the management of hospital-acquired pneumonia in the UK. JAC 2008;62:5-34
Pneumocystis jirovecii pneumonia (PJP)
Pneumocystis jirovecii pneumonia (PJP)
- Discussion with Microbiology recommended.
- Co-trimoxazole in high dosage is the treatment of choice for mild, moderate and severe PJP.
- For moderate to severe disease (Pa02 ≤9kPa on room air), high dose steroids should be co-administered with anti-pneumocystis therapy and should be discontinued before anti-pneumocystis therapy is complete: Prednisolone 40mg PO twice daily for 5 days, then 40mg once daily for 5 days, then 20mg once daily to complete a total of 14 to 21 days (depending on duration of PJP treatment).
|
PJP Treatment |
|||
|
Infection |
1 st Line |
2 nd line |
Comment |
|
PJP |
Co-trimoxazole * IV/PO 120mg/kg/ day divided into a 6 to 8 hourly dosing regimen e.g. 30mg/kg every 6 hours * e.g. 70kg patient: 70x120mg = 8,400mg daily, dosing regimen would be 2,100mg every 6 hours (round dose to nearest 480mg vial=1920mg) In severe disease consider oral switch at same dose when clinically improving. In mild to moderate disease consider oral route from outset. |
Severe disease: Pentamidine IV 4mg/kg once daily Please discuss with Microbiology. Only to be used if intolerant or unresponsive to co- trimoxazole. Risk of significant adverse events including severe hypotension and hypoglycaemia with administration. Non-severe disease: Atovaquone OR Dapsone + Trimethoprim OR Clindamycin + Primaquine Contact Microbiology or Pharmacy for advice and dosing. |
Duration (Micro consult recommended): Non-HIV infected: 14 to 21 days HIV infected: 21 days |
|
* Please note the co-trimoxazole dose is a combined trimethoprim/sulfamethoxazole dose. Caution with dose calculation as errors have occurred when dosing is based on the trimethoprim component (as recommended in US literature). |
|||
- Catherinot et al. Pneumocystis jirovecii pneumonia. Infect Dis Clin North Am 2009;24:107-138
Sepsis - Source Unclear
Sepsis - Source Unclear
- Discussion with Microbiology recommended .
- If source is known or suspected e.g. meningitis, respiratory, urinary, skin and soft tissue, ensure antibiotics are appropriate for the source. Follow the antibiotic recommendations in the corresponding chapter.
- Identify need for further intervention to address the source of infection e.g. drainage or removal of source.
- The regimens below may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. See note on MDRO .
- The Sepsis Screening Form should be completed in response to early warning score alerts for infection. Sepsis Six, including first dose antimicrobials, to be completed within one hour of diagnosis of sepsis. See HSE Sepsis Programme resources for further information.
- If infection site is known, culture results are available, and/or patient improved, review treatment with new information and consider de-escalation. If antibiotics are still required, use the narrowest spectrum of coverage for the shortest time.
- Duration of treatment is decided on a case-by-case basis depending on subsequent diagnosis as well as clinical progress.
|
Empiric Antibiotics for Sepsis – Source Unclear |
|||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
|
See penicillin hypersensitivity section for further information |
|||
|
The regimens below may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. See note on MDRO . |
|||
|
If haemodynamically unstable |
Antibiotics must be given as soon as possible, then discuss with Microbiology. Meropenem should be considered in patients who are critically ill with sepsis or have a history of a Gram-negative Multi-drug Resistant Organism (MDRO). Discuss use of Meropenem with Microbiology. If meropenem is essential in a patient with a history of severe penicillin allergy e.g. anaphylaxis, close monitoring is required for cross sensitivity. |
||
|
Sepsis – Source Unclear No risk factors for MRSA e.g. No CVC/ No IV Drug Use |
Give antibiotics immediately |
||
|
Piperacillin/tazobactam IV
+ Gentamicin IV one dose per LAPP App calculator. See footnote 1 re further doses and monitoring. See footnote 2 re use in pregnancy. See footnote 3 re sepsis in pregnancy.
|
CefTRIAXone IV
+ Gentamicin IV one dose per LAPP App calculator. See footnote 1 re further doses and monitoring. See footnote 2 re use in pregnancy. If pregnant or suspected intra-abdominal source: Add
Metronidazole IV
See footnote 3 re sepsis in pregnancy. |
Discuss with Microbiology
Ciprofloxacin
IV
See footnote 2 re use in pregnancy. + Gentamicin IV one dose per LAPP App calculator. See footnote 1 re further doses and monitoring. See footnote 2 re use in pregnancy. + Vancomycin IV infusion, dose per LAPP App calculator. See footnote 1 re monitoring. If pregnant or suspected intra-abdominal source: Add
Metronidazole IV
See footnote 3 re sepsis in pregnancy. |
|
|
Sepsis – Source Unclear CVC in situ/ Inflammation at intravascular catheter insertion site/IV Drug Use/ Risk factors for MRSA |
Give antibiotics immediately |
||
|
Piperacillin/tazobactam IV
+ Gentamicin IV one dose per LAPP App calculator. See footnote 1 re further doses and monitoring. See footnote 2 re use in pregnancy. + Vancomycin IV infusion, dose per LAPP App calculator. See footnote 1 re monitoring. See footnote 3 re sepsis in pregnancy.
|
CefTRIAXone IV
+ Gentamicin IV one dose per LAPP App calculator. See footnote 1 re further doses and monitoring. See footnote 2 re use in pregnancy. + Vancomycin IV infusion, dose per LAPP App calculator. See footnote 1 re monitoring.
If pregnant or suspected intra-abdominal source:
Add
See footnote 3 re sepsis in pregnancy. |
||
|
1 Review need for ongoing Gentamicin and Vancomycin on a daily basis. Continue with once daily Gentamicin dosing ONLY if recommended by patient's Consultant/Registrar . For advice on monitoring see Aminoglycoside & Vancomycin Dosing & Monitoring section. 2 Gentamicin & Ciprofloxacin are recommended in pregnancy when benefit outweighs risk. 3 For full detailed guidance on the management of sepsis in a pregnant patient, see WAC Directorate Guideline on the Management of Suspected Sepsis and Sepsis in Obstetric Care (Available via QPulse Knowledge base CLN-OGCP-218 on Linkopolis). Discuss with Obstetrics. |
|||
References:
- Surviving Sepsis Campaign International Guidelines for Management of Sepsis and Septic Shock 2016
- NCEC Sepsis Management National Clinical Guideline No. 6 2014
- The Sanford Guide to Antimicrobial Therapy Digital Update Feb 2021
- HSE Sepsis programme documents and resources: https://www.hse.ie/eng/about/who/cspd/ncps/sepsis/resources/
Suspected Meningococcaemia (without features of meningitis)
Suspected Meningococcaemia (without features of meningitis)
- Discussion with Microbiology recommended.
- When infection with susceptible N. meningitidis is confirmed, therapy with Benzylpenicillin alone is appropriate.
- Chloramphenicol is available in the Emergency Department and in the Pharmacy Department. Meropenem may be an alternative to chloramphenicol in patients with a history of penicillin anaphylaxis, as recommended in Irish guidelines, with close monitoring for cross-sensitivity.
- See Appendix 4 for management of contacts.
|
Empiric Antibiotics for Suspected Meningococcaemia |
||||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
|
See penicillin hypersensitivity section for further information |
||||
|
Suspected Meningoccaemia (without features of meningitis) |
CefTRIAXone IV 2g every 12 hours |
CefTRIAXone IV 2g every 12 hours |
Give first dose Chloramphenicol IV 25mg/kg and IMMEDIATELY discuss with Microbiology to discuss options.
Meropenem 2g every 8 hours may be an alternative to chloramphenicol in patients with a history of penicillin anaphylaxis, as recommended in Irish guidelines, with close monitoring for cross-sensitivity. Please discuss with microbiology. Discuss need for nasopharyngeal eradication for the patient with Microbiology. |
Duration 7 days |
Skin and Soft Tissue
Skin and Soft Tissue Infections
Skin and Soft Tissue Infections
- The regimens below may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. Vancomycin may be required in addition i.e. if the person’s methicillin-resistant Staphylococcus aureus (MRSA) status if known. See note on MDRO .
- Blood cultures should be performed before starting antimicrobial treatment if at all possible for a patient with a severe infection, especially if the patient is systemically ill.
- Cellulitis must be differentiated from lower leg eczema, oedema with blisters, acute venous problems including deep venous thrombosis (DVT), thrombophlebitis and vasculitis. Bilateral leg cellulitis is extremely rare and other diagnoses, such as bilateral varicose eczema, should be considered. Normal CRP and WCC makes cellulitis less likely.
-
Consider taking a swab for microbiological testing from people with cellulitis or erysipelas to guide treatment, but only if the skin is broken and:
- there is a penetrating injury or
- there has been exposure to water-borne organisms or
- the infection was acquired outside of Ireland
- Before treating cellulitis, consider drawing around the extent of the infection with a single-use surgical marker pen to monitor progress. Be aware that redness may be less visible on darker skin tones.
-
When choosing an antibiotic, take account of:
- the severity of symptoms
- the site of infection (for example, near the eyes or nose)
- the risk of uncommon pathogens (for example, from a penetrating injury, after exposure to water-borne organisms, or an infection acquired outside of Ireland)
- previous microbiological results from a swab e.g. MRSA
- In diabetes, all foot wounds are likely to be colonised with bacteria. Ulcers without any local or systemic signs of infection do not require antibiotic therapy. Antibiotics do not accelerate wound healing of uninfected ulcers.
- Please avoid the prescription of antibiotics and submission of swabs for uninfected ulcers.
|
Empiric Antibiotics for Skin and Soft Tissue Infections |
||||
|
The regimens below may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. Vancomycin may be required in addition to cover MRSA. See note on MDRO . |
||||
|
Cellulitis/Wound Infection |
||||
|
|
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: Immediate or severe delayed reaction |
Comment |
|
Mild |
Flucloxacillin PO 1 1g every 6 hours
|
CefALEXin PO 500mg every 6 hours |
Clarithromycin
|
Duration 5-7 days If a patient requires an extended course please discuss with Microbiology |
|
Moderate - Severe |
Flucloxacillin IV
|
CefAZOLin (Unlicensed) IV 2g every 8 hours |
Clindamycin IV 900mg every 8 hours |
Duration 7-10 days If a patient requires an extended course please discuss with Microbiology |
|
Incipient necrotising fasciitis
|
Discuss urgently with Consultant Microbiologist |
|||
|
Flucloxacillin IV 2g every 6 hours + Clindamycin IV 900mg every 8 hours |
Vancomycin 2 IV infusion, dose per LAPP App calculator. See footnote 2 re monitoring. + Clindamycin IV 900mg every 8 hours |
Duration 7-10 days If a patient requires an extended course please discuss with Microbiology |
||
|
For severe cellulitis and incipient necrotising fasciitis , if involving abdominal wall or groin or water exposure, consider adding Ciprofloxacin IV 400mg every 12 hours |
||||
|
Necrotising fasciitis/gas gangrene (Group A Streptococcal infection) Immediate surgical debridement is essential Discuss immediately with Consultant Microbiologist |
Piperacillin/tazobactam IV 4.5g every 6 hours + Clindamycin IV 1.2g every 6 hours
For MRSA Add Vancomycin 2 IV infusion, dose per LAPP App calculator. See footnote 2 re monitoring. |
Discuss with Microbiology Consider Vancomycin 2 IV infusion, dose per LAPP App calculator. See footnote 2 re monitoring. + Clindamycin IV 1.2g every 6 hours + Ciprofloxacin IV 400mg every 8 hours
Monitor for diarrhoea |
Duration Usual duration 14 days |
|
|
Orbital and Periorbital Cellulitis ( Seek Specialist ENT or Ophthalmology advice urgently ) Treat non-orbital facial cellulitis as cellulitis. |
||||
|
|
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: Immediate or severe delayed reaction |
Comment |
|
Mild |
Co-amoxiclav PO 625mg every 8 hours + Amoxicillin PO 500mg every 8 hours |
CefALEXin PO 500mg every 6 hours + Metronidazole PO 400mg every 8 hours |
Clarithromycin PO 500mg every 12 hours + Metronidazole PO 400mg every 8 hours |
Duration 7 days |
|
Moderate-Severe
Please consider discussing with Microbiology |
CefTRIAXone IV 2g every 24 hours + Metronidazole IV 500mg every 8 hours + Flucloxacillin IV 2g every 6 hours
|
CefTRIAXone IV 2g every
+ Metronidazole IV 500mg every 8 hours + Vancomycin 2 IV infusion, dose per LAPP App calculator. See footnote 2 re monitoring.
|
Vancomycin 2 IV infusion, dose per LAPP App calculator. See footnote 2 re monitoring. +
Clindamycin
IV 900mg every
+
Ciprofloxacin
IV 400mg every
Monitor for diarrhoea. |
Duration 10 to 14 days |
|
Diabetic Soft Tissue Infection (without osteomyelitis) |
||||
|
|
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: Immediate or severe delayed reaction |
Comment |
|
Mild |
Co-amoxiclav PO 625mg every 8 hours + Amoxicillin PO 500mg every 8 hours |
CefUROXime PO 500mg every 12 hours + Metronidazole PO 400mg every 8 hours |
Clindamycin PO 450mg every 6 hours + Ciprofloxacin PO 500mg every 12 hours Monitor for diarrhoea |
Duration: Minimum 7 days |
|
Moderate |
Co-amoxiclav IV 1.2g every 8 hours |
CefUROXime IV 1.5g every 8 hours + Metronidazole IV 500mg every 8 hours
|
Clindamycin
IV
+
Ciprofloxacin
IV
Monitor for diarrhoea |
Duration: 10-14 days in Moderate to Severe infection.
May require up to 3 weeks for severe infection. |
|
Severe
Discuss with Consultant Microbiologist. Higher doses may be indicated |
Piperacillin/tazobactam IV 4.5g every 6 hours |
Vancomycin 2 IV infusion, dose per LAPP App calculator. See footnote 2 re monitoring. + Clindamycin IV 900mg every 8 hours + Ciprofloxacin IV 400mg every 12 hours Monitor for diarrhoea Discuss with Microbiology |
||
|
1. The upper dose of Flucloxacillin PO 1g four times a day is unlicensed. 2. Review need for ongoing vancomycin on a daily basis. For advice on monitoring see Vancomycin Dosing & Monitoring section. |
||||
References:
1. IDSA Guidelines for Diagnosis & Management of Skin & Soft-Tissue Infections 2014 Update. Clin Infect Dis 2014
2. IDSA Guidelines for Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis 2012;54:132-173
3. NICE Guideline Diabetic foot problems: prevention and management 2015. Updated 2019 https://www.nice.org.uk/guidance/ng19
4. Lehman. Flucloxacillin alone or combined with benzylpenicillin to treat lower limb cellulitis: a randomised controlled trial. Emerg Med J 2005;22:342-346
5. NICE guideline, Cellulitis and erysipelas: antimicrobial prescribing 2019 https://www.nice.org.uk/guidance/ng141
6. Tallaght University Hospital Adult Medicines Guide, Empiric treatment guidelines, Skin and soft tissue infection. Accessed May 2024
7. Tallaght University Hospital Adult Medicines Guide, Empiric treatment guidelines, Diabetic foot infection. Accessed May 2024
Bites, Animal and Human, Prophylaxis and Treatment
Bites, Animal and Human, Prophylaxis and Treatment
- This guidance provides recommendations on antibiotic choice for prophylaxis and treatment of bite wounds. It is not a comprehensive guide to the care of bite wounds. Other factors which need to be considered in addition to antibiotic choice include the nature of the injury, the type of bite, the country in which the bite occurred and previous immunization history issues such as prophylaxis against HIV infection and immunization against tetanus, hepatitis B and rabies. Refer to HSE immunisation guideline chapters on tetanus and rabies for risk assessment and management. Refer to Guidelines for the Emergency Management of Injuries (EMI) and Post-Exposure Prophylaxis (PEP) March 2024 for information on management of infection risk from a blood borne virus (BBV) following Human Bite breaching skin- or ‘fight bite’.
- Application of topical antiseptics is NOT of value and should be avoided. Sterile water is appropriate for wound irrigation.
- Antibiotic prophylaxis is generally NOT appropriate for animal bites more than 2 days old OR human bites more than 3 days old at time of presentation.
- Antibiotic prophylaxis is appropriate for:
- All human bites less than 3 days old, all cat bites less than 2 days old and other animal bites less than 2 days old to the hand, foot and face; puncture wounds; wounds that require surgical debridement or involving joints, tendons, ligaments or fractures.
- Wounds that have undergone primary closure.
- People at risk of serious wound infection (e.g. those who are immunocompromised, diabetic, asplenic or cirrhotic).
- People with a prosthetic valve or prosthetic joint.
5. If there are signs of infection, the issue is one of treatment rather than prophylaxis. In the absence of previous appropriate prophylaxis the regimens below are generally appropriate for treatment of infected bites; however the dose, route of administration and choice of agents may require adjustment based on severity of infection.
6. Seek specialist advice (discuss with consultant microbiologist) for bites from a wild or exotic animal (including birds) as they may require different antimicrobial cover and there may be a risk of other serious non-bacterial infections.
|
Empiric Antibiotics for Animal and Human Bites |
|||
|
Infection |
1 st line Antibiotics |
In penicillin allergy |
Comment |
|
Animal & human bites, prophylaxis and treatment |
Co-amoxiclav PO 625mg every 8 hours
|
Metronidazole PO 400mg every 8 hours + Doxycycline PO 100mg every 12 hours |
Duration: Prophylaxis - 3 days Treatment* - 5 days *Treatment duration can be increased to 7 days if there was significant tissue destruction or the wound has penetrated bone, joint, tendon or vascular structures. Such wounds would require surgical management Consider need for IV therapy or longer duration if severe infection |
References:
-
Bites (Human and Animal). Comments from Expert Advisory Committee. HSE Antibiotic prescribing Guidelines for Treatment of Community Infections. Accessed October 2024. ( https://www.hse.ie/eng/services/list/2/gp/antibiotic-prescribing/conditions-and-treatments/skin-soft-tissue/human-bite/)
- Guidelines for the Emergency Management of Injuries (EMI) and Post-Exposure Prophylaxis (PEP) March 2024. Accessed March 2024 ( https://www.hpsc.ie/a-z/emi/ )
- NIAC Immunisation Guidelines for Ireland. https://www.rcpi.ie/Healthcare-Leadership/NIAC/Immunisation-Guidelines-for-Ireland
Throat
Throat
- Antibiotic therapy is generally NOT indicated for acute pharyngitis/tonsillitis in the community as most throat infections are viral .
- This recommendation is for patients requiring hospitalisation.
- Avoid Amoxicillin and co-amoxiclav if glandular fever is considered likely.
- If condition is considered life threatening treat as for acute epiglottitis.
-
The
FeverPAIN scoring system
can help identify those who are most likely to benefit from antibiotics.
- Higher scores suggest more severe symptoms and likely bacterial (streptococcal) cause.
-
FeverPAIN criteria [each of the FeverPain criteria score 1 point (maximum score of 5)]:
- Fever
- Pus on tonsils
- Attendance within 3 days of onset of symptoms
- Severely inflamed tonsils
- No cough or coryzal symptoms present
Score 0-1: Do not offer antibiotic
Score 2-3: Offer delayed antibiotic
Score 4-5: Offer immediate antibiotic prescription
|
Empiric Antibiotics for Throat Infections |
||||
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
|
See penicillin hypersensitivity section for further information |
||||
|
Acute Pharyngitis/ Tonsillitis |
Benzylpenicillin IV 1.2g every 4 hours
If there is a good response to initial IV therapy consider switch to oral therapy with: Phenoxymethylpenicillin PO 666mg every 6 hours OR Amoxicillin PO 500mg every 8 hours |
Clarithromycin IV 500mg every 12 hours Consider switch to oral therapy if good response to initial IV therapy |
Duration 10 days.
Consider switch to oral agents after 24-48 hours.
If failure to respond to initial therapy consider: Co-amoxiclav IV 1.2g every 8 hours (if no allergy to penicillin). |
|
|
Peritonsillar abscess Discuss with ENT re early surgical drainage of abscess |
Co-amoxiclav IV 1.2g every 8 hours |
CefTRIAXone 2g every 24 hours + Metronidazole IV 500mg every 8 hours |
Clindamycin IV 900mg every 8 hours |
Duration usually 7 days. Consider oral switch when appropriate -discuss with Micro. |
|
Severe Acute Epiglottitis Discuss with Microbiology |
CefTRIAXone IV 2g every 24 hours |
CefTRIAXone IV 2g every 24 hours |
Vancomycin IV infusion, dose per LAPP App calculator. See footnote* re monitoring. + Ciprofloxacin IV 400mg every 12 hours |
Optimal duration of treatment not established. Generally treat for 7-10 days. Longer duration may be indicated in selected patients. Consider oral switch when appropriate - discuss with Microbiology. |
|
* For advice on monitoring see Vancomycin Dosing & Monitoring section. |
||||
References:
1. The Sanford Guide to Antimicrobial Therapy Digital Update Accessed online January 2025
2. Shulman et al IDSA Practice Guidelines for the Diagnosis and Management of Group A Streptococcal Pharyngitis Clin Infect Dis 2012;55:e86-102
3. Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America
4. HSE Antimicrobial Resistance and Infection Control Programme Version 2.2 Reviewed: March 2026. Accessed March 2026 via chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://assets.hse.ie/media/documents/Pharyngitis_sore_throat_tonsillitis_guideline.pdf
Urinary Tract
Urinary Tract Infections
Urinary Tract Infections
- Non-pregnant patients with asymptomatic bacteriuria do NOT require antibiotic treatment.
- Bacteriuria in a patient with an indwelling urinary catheter is NOT an indication for treatment unless there are specific clinical features of infection. Removal of the urinary catheter at the earliest possible time is the best approach to dealing with catheter-associated bacteriuria. Contact Urology where appropriate.
- A practice of routine antimicrobial prophylaxis with gentamicin or other agents at the time of catheterisation is NOT appropriate. See surgical prophylaxis section for note related to recent urological surgery .
- Multi-drug resistant organisms (MDRO) are relatively common in patients with UTI from a nursing home setting and increasingly in other patients. Review recent previous urine culture and sensitivity. See note on ESBL and MDRO .
- The use of dipstick urinalysis in assessing for evidence of a UTI is not a useful guide to management and is not recommended for all persons aged 65 years and older AND all persons with an indwelling catheter. Inappropriate use of dipsticks can lead to unnecessary antibiotic prescribing which does not benefit the patient and may cause considerable harm including adverse effects, drug interactions, and antimicrobial resistance. Please see National HSE guidelines for more information.
- These are summary empiric antibiotic choices for adult patients. If pregnancyFull detailed Women’s and Children’s (WAC) Group Management of Urinary Tract Infections (UTI’s) in Pregnancy (CLN-QGCP-227) are available via Linkopolis→ HCI-QPulse Knowledgebase→ PPG Library.
|
Empiric Antibiotics for Urinary Tract Infections |
||||
|
Infection |
1 st Line Antibiotics |
Comment |
Duration |
|
|
The regimens below may NOT cover Multi-drug Resistant Organisms (MDRO) in all cases. See note on MDRO . |
||||
|
Non-pregnant Females & Males Cystitis/Lower UTI (i.e. uncomplicated UTI) |
Nitrofurantoin PO
(immediate
release
preparation)
Avoid nitrofurantoin if eGFR <45ml/min/1.73m
2
.
Alternative 1 st choice option ( only if nitrofurantoin unsuitable) : CeFALexin PO 500mg every 8 to 12 hours
OR
Trimethoprim PO 200mg every 12 hours
|
Adjust initial treatment based on culture & sensitivity results. Please ensure pre-treatment MSU in males sent .
If eGFR <45ml/min/1.73m 2 and penicillin allergic please discuss patients with Microbiology.
If pregnant , see Saolta full detailed guideline WAC Group Management of Urinary Tract Infections (UTIs) in Pregnancy (available via Linkopolis > HCI-QPulse Knowledgebase > PPG Library > Women’s & Children’s Directorate and search CLN-OGCP-227) or please discuss with microbiology.
Important to note for men:
|
Duration for non-pregnant women : 3 days *
Duration for
males
:
*Note: If history of recurrent infection or inadequate treatment response, consider extending treatment to 5 days. |
|
|
Catheter associated UTI (Lower UTI/not systemically unwell) Refers to patients (male/female) whose urinary tract is currently catheterised or has been catheterised within the past 48hours.
For Upper catheter associated UTI / systemically unwell please see below under “Complicated UTI”.
|
Nitrofurantoin PO
(immediate
release
preparation)
Avoid nitrofurantoin if eGFR <45ml/min/1.73m
2
.
Alternative 1 st choice option ( only if nitrofurantoin is unsuitable):
CeFALexin PO 500mg every 8 to 12 hours
OR
Trimethoprim PO 200mg every 12 hours
|
Adjust initial treatment based on culture & sensitivity results. If eGFR <45ml/min/1.73m 2 and penicillin allergic please discuss patients with Microbiology.
Note indwelling urethral or suprapubic catheters often become colonised with bacteria without signs of symptoms of infection in the patient. Antibiotic treatment is of no benefit in these patients.
Antibiotic prophylaxis for urinary catheter changes is NOT appropriate unless there is a definite history of UTI due to catheter change.
|
7 days |
|
|
Infection |
1 st Line Antibiotics |
Penicillin allergy: delayed onset non-severe reaction |
Penicillin allergy: immediate or severe delayed reaction |
Comment |
|
See penicillin hypersensitivity section for further information |
||||
|
Pyelonephritis or Complicated UTI Non-pregnancy Consider acute pyelonephritis/upper UTI when:
|
< 50 years with minimal previous exposure to
Co-amoxiclav IV 1.2g every 8 hours + Gentamicin IV one dose per LAPP App calculator. See footnote* re further doses and monitoring. If a patient continues to be haemodynamically unstable continue gentamicin guided by trough levels. Please consult the gentamicin calculator , microbiologist or pharmacy for dosing information as needed.
>50 years and/or extensive previous exposure to antibitoics: Piperacillin/tazobactam IV 4.5g every 8 hours + Gentamicin IV one dose per LAPP App calculator. See footnote* re further doses and monitoring. If a patient continues to be haemodynamically unstable continue gentamicin guided by trough levels. Please consult the gentamicin calculator , microbiologist or pharmacy for dosing information as needed.
If patient is septic and/or acutely unwell discuss with Microbiology. |
CefTRIAXone IV 2g every 24 hours
Add
Gentamicin
IV
IF
|
Ciprofloxacin IV 400mg (or PO 500mg) every 12 hours (consider oral route from outset) (See Fluroquinolone warning)
Add
Gentamicin
IV
|
Minimum duration of treatment is 10 days.
Consider switch to oral therapy if good early clinical response to IV therapy. Please see chapter on IV to PO switch for more information. Review need for continuing Gentamicin after 24 hours. |
|
Acute Pyelonephritis In pregnancy |
If pregnant, see Saolta full detailed guideline WAC Group Management of Urinary Tract Infections (UTIs) in Pregnancy (available via Linkopolis > HCI-QPulse Knowledgebase > PPG Library > Women’s & Children’s Directorate and search CLN-OGCP-227). |
|||
|
CefTRIAXone IV 2g every 24 hours
Add
Gentamicin
IV
IF
|
Gentamicin IV every 24 hours, dose per LAPP App calculator (use booking weight). See footnote* re review and monitoring. See footnote^ re use in pregnancy. + Either (depending on Group B Streptococcus susceptibility result if available)
Vancomycin
IV infusion, dose per LAPP App calculator (use booking weight). See footnote*
OR Clindamycin IV 900mg every 8 hours Give first doses, THEN IMMEDIATELY discuss with Microbiology to discuss further therapy. |
|||
|
^ Gentamicin is recommended in pregnancy when benefit outweighs risk. * Review need for ongoing Gentamicin and Vancomycin on a daily basis. Continue with once daily Gentamicin dosing ONLY if Consultant/Registrar recommended. For advice on monitoring see Aminoglycoside & Vancomycin Dosing & Monitoring section. |
||||
References:
- IDSA/ESCMID Guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women. Clin Infect Dis 2011;52:e103-e120
- SIGN 88: Management of suspected bacterial urinary tract infection in adults July 2012
- Women’s and Children’s (WAC) Group Management of Urinary Tract Infections (UTI’s) in Pregnancy (QPulse CLN-OGCP-227)
- NICE guideline NG109 Urinary tract infection (lower): antimicrobial prescribing Published 31 October 2018
- NICE guideline NG113 Urinary tract infection (catheter associated): antimicrobial prescribing. Published 23 November 2018
- AMRIC Urinary guidelines Antibiotic Prescribing - Conditions and Treatments - HSE.ie (Accessed May 2024)
Prophylaxis of Recurrent Urinary Tract Infections
Prophylaxis of Recurrent Urinary Tract Infections
Discussion with Microbiology is recommended .
In the absence of a correctable anatomical or other predisposing factor for recurrent UTI, prophylaxis for a period of 3 to 6 months may be considered. There is no evidence of any additional benefit from such prophylaxis beyond 3-6 months. In fact, there is significant evidence of harm. Please see HSE AMRIC guidance for more information. The patient should be advised upon initiation that antibiotic prophylaxis is prescribed for a fixed period of time, that there is a risk of side effects and that this is not intended to be a long-term medication.
In general the most appropriate agent for prophylaxis is nitrofurantoin PO 50mg to 100 mg at night.
CAUTION: Continuation of nitrofurantoin is very rarely justified and if considered should be discussed with Microbiology. Chronic pulmonary reactions and chronic active hepatitis, occasionally leading to hepatic necrosis, can occur rarely in patients treated with nitrofurantoin. They are generally associated with long-term therapy (usually after six months). If an ongoing need for antibiotic prophylaxis is required post 6-month exposure to nitrofurantoin, an alternative antibiotic is advised where possible. Monitor lung and liver function in patients on long-term nitrofurantoin therapy. Avoid in renal impairment (eGFR less than 45ml/minute when used as prophylaxis).
References:
- HSE Antimicrobial Resistance and Infection Control (AMRIC) group: Antibiotic Prescribing - Deprescribing UTI prophylaxis guidance. Updated November 2023 (Accessed March 2024) Deprescribing UTI prophylaxis - HSE.ie
- IDSA/ESCMID Guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women. Clin Infect Dis 2011;52:e103-e120
- SIGN 160: Management of suspected bacterial urinary tract infection in adults Sept 2020
Viral
Viral
|
Treatment of Viral Infections |
||
|
Infection |
Treatment |
Comment |
|
Herpes simplex - Cold sores |
Aciclovir 5% cream every 4 hours
|
Most effective when applied at the earliest possible stage - at prodromal stage before vesicles appear. Systemic treatment is necessary if frequent recurrences or for extensive infections. |
|
Herpes simplex – Including Mouth/lips and Genital herpes |
Treatment: ValACIclovir PO 500mg every 12 hours (1g every 12 hours in immunocompromised)
Initial duration: Treat for 5 to 10 days (10 days duration in immunocompromised)
If Recurrent: Treat for 3 to 5 days (5 to 10 days in immunocompromised) Suppression: ValACIclovir PO 500mg every 24 hours (500mg every 12 hours in immunocompromised), therapy to be interrupted every 6 to 12 months to reassess recurrence frequency. |
If IV treatment needed e.g. herpes simplex in immunocompromised, severe genital herpes or prophylaxis in immunocompromised: Aciclovir IV 5mg/kg every 8 hours. Higher dose may be required in severe infection/immunocompromised. Discuss with Microbiology. |
|
Herpes zoster (shingles) |
ValACIclovir PO 1g every 8 hours for 7 days (in immunocompromised continue for 2 days after crusting of lesions) |
If IV treatment needed: Aciclovir IV 5mg/kg every 8 hours (10mg/kg every 8 hours in immunocompromised). If disease is severe i.e. ocular, neurologic, disseminated disease or immunocompromised discuss with Microbiology. |
|
Herpes simplex encephalitis |
||
References:
- British Association of Sexual Health and HIV UK national guideline for the management of anogenital herpes, 2024 [Accessed March 2026]
- The Sanford Guide to Antimicrobial Therapy Digital Update Feb 2018
- HSE Antibiotic prescribing Genital Herpes [Accessed January 2025]
- BNF Valaciclovir https://doi.org/10.18578/BNF.947433078 [Last Update: 23-Sep-2022]